
Understanding the Relationship between Fetal Alcohol Spectrum Disorder (FASD) and Criminal Justice: A Systematic Review

 ,
, 
 ,
,  ,
, 
Abstract
:1. Introduction
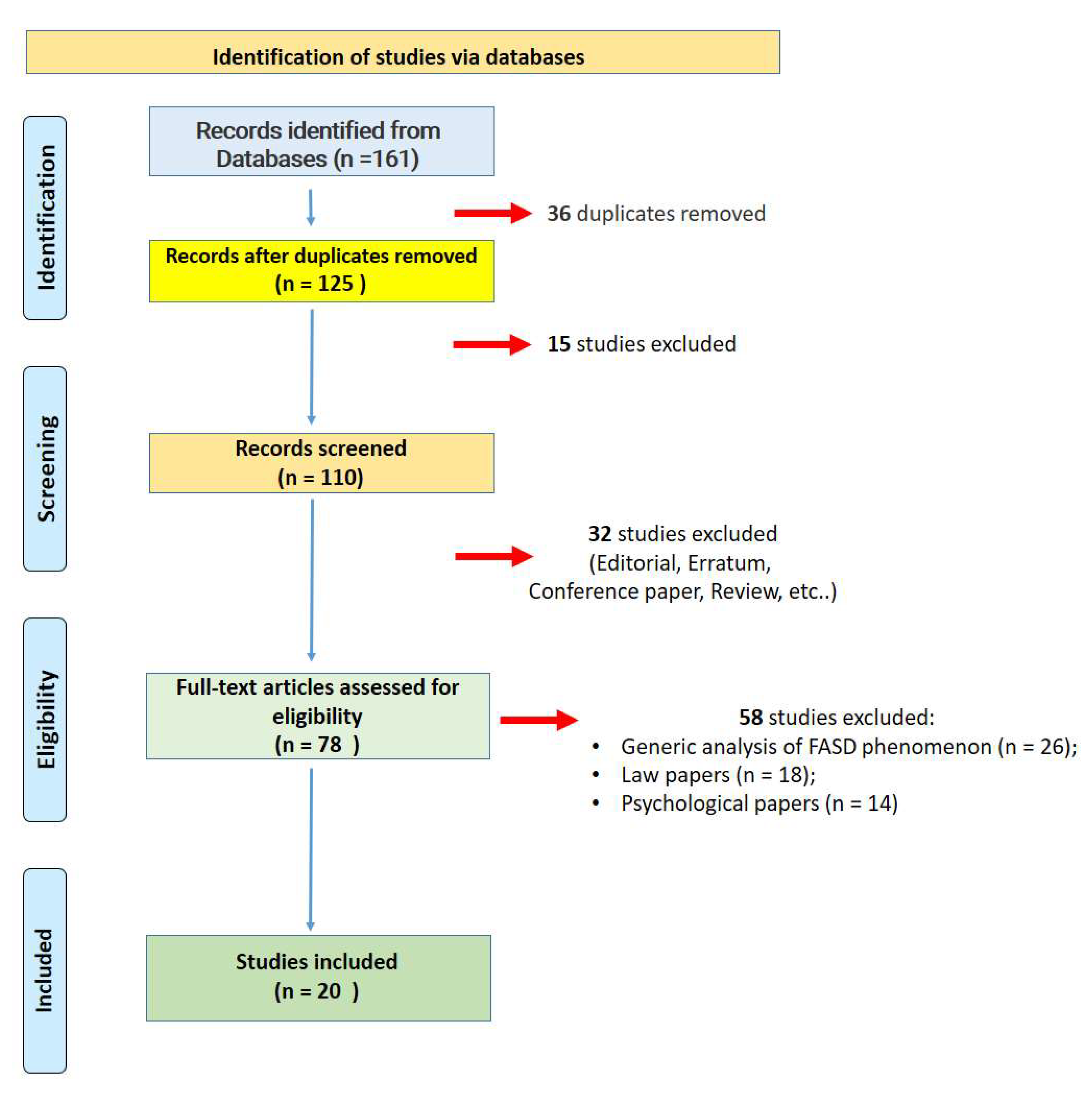
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Quality Assessment and Data Extraction
2.3. Risk of Bias
2.4. Characteristics of Eligible Studies
3. Results
3.1. FASD Subjects and Brain Impairment
3.2. FASD Subjects in Indigenous Group
3.3. FASD Subjects and Justice System
4. Discussion
- -
- to adopt specific training for police, courts staff, lawyers and other stakeholders in order to illustrate the complex FASD phenomenon;
- -
- to constitute a multidisciplinary group to promptly identify subjects with FASD to conduct a fair trial;
- -
- to carry out research studies both to better define the possible incidence of FASD in the prison population and to establish targeted support interventions in prison to prevent recidivism;
- -
- to activate a follow-up for all prisoners diagnosed with FASD.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dozet, D.; Burd, L.; Popova, S. Screening for Alcohol Use in Pregnancy: A Review of Current Practices and Perspectives. Int. J. Ment. Health Addict. 2021, 1–20. [Google Scholar] [CrossRef]
- Popova, S.; Lange, S.; Probst, C.; Gmel, G.; Rehm, J. Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e290–e299. [Google Scholar] [CrossRef] [Green Version]
- Clarke, M.E.; Gibbard, W.B. Overview of fetal alcohol spectrum disorders for mental health professionals. Can. Child Adolesc. Psychiatr. Rev. 2003, 12, 57–63. [Google Scholar]
- Benz, J.; Rasmussen, C.; Andrew, G. Diagnosing fetal alcohol spectrum disorder: History, challenges and future directions. Paediatr. Child Health 2009, 14, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Cook, J.L.; Green, C.R.; Lilley, C.M.; Anderson, S.M.; Baldwin, M.E.; Chudley, A.E.; Conry, J.L.; LeBlanc, N.; Loock, C.A.; Lutke, J.; et al. Fetal alcohol spectrum disorder: A guideline for diagnosis across the lifespan. CMAJ 2016, 188, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.M.; Haun, J.; Zapf, P.A.; Brown, N.N. Fetal Alcohol Spectrum Disorders (FASD) and competency to stand trial (CST): Suggestions for a “best practices” approach to forensic evaluation. Int. J. Law Psychiatry 2017, 52, 19–27. [Google Scholar] [CrossRef]
- Makela, M.; Kapasi, A.; Pei, J.; Mcfarlane, A. Supporting Employment in Individuals with FASD: A Guide for Employment Professionals; PolicyWise for Children & Families: Edmonton, AB, Canada; Canada FASD Research Network: Vancouver, BC, Canada; University of Alberta: Edmonton, AB, Canada, 2018. [Google Scholar]
- Petrenko, C.L.M.; Tahir, N.; Mahoney, E.C.; Chin, N.P. Prevention of secondary conditions in fetal alcohol spectrum disorders: Identification of systems-level barriers. Matern. Child Health J. 2014, 18, 1496–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senturias, Y.S.N. Fetal alcohol spectrum disorders: An overview for pediatric and adolescent care providers. Curr. Probl. Pediatr. Adolesc. Health Care 2014, 44, 74–81. [Google Scholar] [CrossRef]
- Flannigan, K.; Pei, J.; Stewart, M.; Johnson, A. Fetal Alcohol Spectrum Disorder and the criminal justice system: A systematic literature review. Int. J. Law Psychiatry 2018, 57, 42–52. [Google Scholar] [CrossRef]
- Rangmar, J.; Hjern, A.; Vinnerljung, B.; Strömland, K.; Aronson, M.; Fahlke, C. Psychosocial outcomes of fetal alcohol syndrome in adulthood. Pediatrics 2015, 135, e52–e58. [Google Scholar] [CrossRef]
- Popova, S.; Lange, S.; Burd, L.; Rehm, J. Burden and Social Cost of Fetal Alcohol Spectrum Disorders; Oxford University Press: Oxford, UK, 2016; Volume 1, ISBN 9780199935291. [Google Scholar]
- Popova, S.; Lange, S.; Burd, L.; Chudley, A.E.; Clarren, S.K.; Rehm, J. Cost of fetal alcohol spectrum disorder diagnosis in Canada. PLoS ONE 2013, 8, e60434. [Google Scholar] [CrossRef] [Green Version]
- Ericson, L.; Magnusson, L.; Hovstadius, B. Societal costs of fetal alcohol syndrome in Sweden. Eur. J. Health Econ. 2017, 18, 575–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stade, B.; Ali, A.; Bennett, D.; Campbell, D.; Johnston, M.; Lens, C.; Tran, S.; Koren, G. The burden of prenatal exposure to alcohol: REVISED measurement of cost. Can. J. Clin. Pharmacol. 2009, 16, 91–102. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Widder, M.; Mierzwa, L.; Schwerg, L.; Schecke, H.; Kornhuber, J.; Bouna-Pyrrou, P.; Bumb, J.M.; Richter-Schmidinger, T.; Lenz, B. Evaluation of the German biographic screening interview for fetal alcohol spectrum disorder (BSI-FASD). Sci. Rep. 2021, 11, 1–9. [Google Scholar]
- Coles, C.D.; Kalberg, W.; Kable, J.A.; Tabachnick, B.; May, P.A.; Chambers, C.D. Characterizing Alcohol-Related Neurodevelopmental Disorder: Prenatal Alcohol Exposure and the Spectrum of Outcomes. Alcohol. Clin. Exp. Res. 2020, 44, 1245–1260. [Google Scholar] [CrossRef]
- Maya-Enero, S.; Ramis-Fernández, S.M.; Astals-Vizcaino, M.; García-Algar, Ó. Neurocognitive and behavioral profile of fetal alcohol spectrum disorder. An. Pediatría Engl. Ed. 2021, 95, 208.e1–208.e9. [Google Scholar] [CrossRef]
- Bühn, S.; Mathes, T.; Prengel, P.; Wegewitz, U.; Ostermann, T.; Robens, S.; Pieper, D. The risk of bias in systematic reviews tool showed fair reliability and good construct validity. J. Clin. Epidemiol. 2017, 91, 121–128. [Google Scholar] [CrossRef]
- Streissguth, A.P.; Bookstein, F.L.; Barr, H.M.; Sampson, P.D.; O’Malley, K.; Young, J.K. Risk factors for adverse life outcomes in Fetal Alcohol Sydnrome and Fetal Alcohol Effects. J. Dev. Behav. Pediatr. 2004, 25, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Cockram, J. Justice or differential treatment? Sentencing of offenders with an intellectual disability. J. Intellect. Dev. Disabil. 2005, 30, 3–13. [Google Scholar] [CrossRef]
- Rojas, E.Y.; Gretton, H.M. Background, offence characteristics, and criminal outcomes of aboriginal youth who sexually offend: A closer look at aboriginal youth intervention needs. Sex. Abus. J. Res. Treat. 2007, 19, 257–283. [Google Scholar] [CrossRef]
- Salmon, J.V.; Buetow, S.A. An exploration of the experiences and perspectives of new zealanders with fetal alcohol spectrum disorder. J. Popul. Ther. Clin. Pharmacol. 2012, 19, 41–50. [Google Scholar]
- Momino, W.; Félix, T.M.; Abeche, A.M.; Zandoná, D.I.; Scheibler, G.G.; Chambers, C.; Jones, K.L.; Flores, R.Z.; Schüler-Faccini, L. Maternal drinking behavior and Fetal Alcohol Spectrum disorders in adolescents with criminal behavior in southern Brazil. Genet. Mol. Biol. 2012, 35, 960–965. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, K.; Roesch, R.; Viljoen, J.L.; Douglas, K.S. Evaluating the psycholegal abilities of young offenders with fetal alcohol spectrum disorder. Law Hum. Behav. 2014, 38, 10–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerji, A.; Shah, C. Ten-year experience of fetal alcohol spectrum disorder; diagnostic and resource challenges in Indigenous children. Paediatr. Child Heath. 2017, 22, 143–147. [Google Scholar] [CrossRef]
- Tait, C.L.; Mela, M.; Boothman, G.; Stoops, M.A. The lived experience of paroled offenders with fetal alcohol spectrum disorder and comorbid psychiatric disorder. Transcult. Psychiatry 2017, 54, 107–124. [Google Scholar] [CrossRef]
- Bower, C.; Watkins, R.E.; Mutch, R.C.; Marriott, R.; Freeman, J.; Kippin, N.R.; Safe, B.; Pestell, C.; Cheung, C.S.C.; Shield, H.; et al. Fetal alcohol spectrum disorder and youth justice: A prevalence study among young people sentenced to detention in Western Australia. BMJ Open 2018, 8, e019605. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, K.; Gray, A.L.; Roesch, R.; Douglas, K.S.; Viljoen, J.L. An evaluation of the predictive validity of the SAVRY and YLS/CMI in justice-involved youth with fetal alcohol spectrum disorder. Psychol. Assess. 2018, 30, 1640–1651. [Google Scholar] [CrossRef] [Green Version]
- McLachlan, K.; McNeil, A.; Pei, J.; Brain, U.; Andrew, G.; Oberlander, T.F. Prevalence and characteristics of adults with fetal alcohol spectrum disorder in corrections: A Canadian case ascertainment study. BMC Public Health 2019, 19, 43. [Google Scholar] [CrossRef] [PubMed]
- Brintnell, E.S.; Sawhney, A.S.; Bailey, P.G.; Nelson, M.; Pike, A.D.; Wielandt, P. Corrections and connection to the community: A diagnostic and service program for incarcerated adult men with FASD. Int. J. Law Psychiatry 2019, 64, 8–17. [Google Scholar] [CrossRef]
- Flannigan, K.; Pei, J.; Burke, A.; Frenzel, R.; Rasmussen, C. Neurocognitive functioning in young offenders with Fetal Alcohol Spectrum Disorder. Int. J. Law Psychiatry 2019, 65, 101347. [Google Scholar] [CrossRef] [PubMed]
- Brownell, M.; Enns, J.E.; Hanlon-Dearman, A.; Chateau, D.; Phillips-Beck, W.; Singal, D.; MacWilliam, L.; Longstaffe, S.; Chudley, A.; Elias, B.; et al. Health, Social, Education, and Justice Outcomes of Manitoba First Nations Children Diagnosed with Fetal Alcohol Spectrum Disorder: A Population-Based Cohort Study of Linked Administrative Data. Can. J. Psychiatry 2019, 64, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Kambeitz, C.; Klug, M.G.; Greenmyer, J.; Popova, S.; Burd, L. Association of adverse childhood experiences and neurodevelopmental disorders in people with fetal alcohol spectrum disorders (FASD) and non-FASD controls. BMC Pediatr. 2019, 19, 498. [Google Scholar] [CrossRef]
- Mela, M.; Flannigan, K.; Anderson, T.; Nelson, M.; Krishnan, S.; Chizea, C.; Takahashi, S.; Sanjanwala, R. Neurocognitive function and fetal alcohol spectrum disorder in offenders with mental disorders. J. Am. Acad. Psychiatry Law 2020, 48, 195–208. [Google Scholar]
- Mullally, K.; McLachlan, K.; MacKillop, E.; Pei, J. Performance validity testing in justice-involved adults with fetal alcohol spectrum disorder. J. Int. Neuropsychol. Soc. 2020, 26, 701–713. [Google Scholar] [CrossRef]
- Hamilton, S.; Reibel, T.; Maslen, S.; Watkins, R.; Jacinta, F.; Passmore, H.; Mutch, R.; O’Donnell, M.; Braithwaite, V.; Bower, C. Disability “In-Justice”: The Benefits and Challenges of “Yarning” With Young People Undergoing Diagnostic Assessment for Fetal Alcohol Spectrum Disorder in a Youth Detention Center. Qual. Health Res. 2020, 30, 314–327. [Google Scholar] [CrossRef]
- Hashmi, S.; Richards, D.; Fedoroff, J.P. A descriptive analysis of sentencing decisions by the Canadian criminal justice system of people with intellectual disabilities convicted with sexual offences. Int. J. Law Psychiatry 2021, 78, 101730. [Google Scholar] [CrossRef] [PubMed]
- Smye, V.; Browne, A.J.; Varcoe, C.; Josewski, V. Harm reduction, methadone maintenance treatment and the root causes of health and social inequities: An intersectional lens in the Canadian context. Harm Reduct. J. 2011, 8, 17. [Google Scholar] [CrossRef] [Green Version]
- Beavis, A.S.W.; Hojjati, A.; Kassam, A.; Choudhury, D.; Fraser, M.; Masching, R.; Nixon, S.A. What all students in healthcare training programs should learn to increase health equity: Perspectives on postcolonialism and the health of Aboriginal Peoples in Canada. BMC Med. Educ. 2015, 15, 155. [Google Scholar] [CrossRef] [Green Version]
- Maar, M.A.; Yeates, K.; Toth, Z.; Barron, M.; Boesch, L.; Hua-Stewart, D.; Liu, P.; Perkins, N.; Sleeth, J.; Wabano, M.J.; et al. Unpacking the Black Box: A Formative Research Approach to the Development of Theory-Driven, Evidence-Based, and Culturally Safe Text Messages in Mobile Health Interventions. JMIR mHealth uHealth 2016, 4, e10. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.; Neal, D.; Carter, M.N.; Louie, J. Sex offender treatment professional perceptions of Fetal Alcohol Spectrum Disorder (FASD) in the Midwest. Int. J. Law Psychiatry 2019, 66, 101476. [Google Scholar] [CrossRef] [PubMed]
- Currie, B.A.; Hoy, J.; Legge, L.; Temple, V.K.; Tahir, M. Adults with fetal alcohol spectrum disorder: Factors associated with positive outcomes and contact with the criminal justice system. J. Popul. Ther. Clin. Pharmacol. 2016, 23, e37–e52. [Google Scholar] [PubMed]
- Tangsermkijsakul, A. Fetal alcohol syndrome in sudden unexpected death in infancy a case report in medicolegal autopsy. Am. J. Forensic Med. Pathol. 2016, 37, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Novick Brown, N.; Greenspan, S. Diminished culpability in fetal alcohol spectrum disorders (FASD). Behav. Sci. Law 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Morini, L.; Marchei, E.; Vagnarelli, F.; Garcia Algar, O.; Groppi, A.; Mastrobattista, L.; Pichini, S. Ethyl glucuronide and ethyl sulfate in meconium and hair-potential biomarkers of intrauterine exposure to ethanol. Forensic Sci. Int. 2010, 196, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Maschke, J.; Roetner, J.; Bösl, S.; Plank, A.-C.; Rohleder, N.; Goecke, T.W.; Fasching, P.A.; Beckmann, M.W.; Kratz, O.; Moll, G.H.; et al. Association of Prenatal Alcohol Exposure and Prenatal Maternal Depression with Offspring Low-Grade Inflammation in Early Adolescence. Int. J. Environ. Res. Public Health 2021, 18, 7920. [Google Scholar] [CrossRef]
- Hastedt, M.; Krumbiegel, F.; Gapert, R.; Tsokos, M.; Hartwig, S. Fatty acid ethyl esters (FAEEs) as markers for alcohol in meconium: Method validation and implementation of a screening program for prenatal drug exposure. Forensic Sci. Med. Pathol. 2013, 9, 287–295. [Google Scholar] [CrossRef]
- Cabarcos, P.; Tabernero, M.J.; Alvarez, I.; Miguez, M.; Fernández, P.; Bermejo, A.M. A new method for quantifying prenatal exposure to ethanol by microwave-assisted extraction (MAE) of meconium followed by gas chromatography-mass spectrometry (GC-MS). Anal. Bioanal. Chem. 2012, 404, 147–155. [Google Scholar] [CrossRef]
- Kulaga, V.; Pragst, F.; Fulga, N.; Koren, G. Hair analysis of fatty acid ethyl esters in the detection of excessive drinking in the context of fetal alcohol spectrum disorders. Ther. Drug Monit. 2009, 31, 261–266. [Google Scholar] [CrossRef]
- Hackler, C. Ethical, legal and policy issues in management of fetal alcohol spectrum disorder. J. Ark. Med. Soc. 2011, 108, 123–124. [Google Scholar]
- Seiler, N.K. Alcohol and Pregnancy: CDC’s Health Advice and the Legal Rights of Pregnant Women. Public Health Rep. 2016, 131, 623–627. [Google Scholar] [CrossRef]
- Supreme Court Judgments. Winnipeg Child and Family Services (Northwest Area); HeinOnline: Buffalo, NY, USA, 1997; Volume 3, p. SCR 925. [Google Scholar]
- Rasmussen, C.; Kully-Martens, K.; Denys, K.; Badry, D.; Henneveld, D.; Wyper, K.; Grant, T. The effectiveness of a community-based intervention program for women at-risk for giving birth to a child with fetal alcohol spectrum disorder (FASD). Community Ment. Health J. 2012, 48, 12–21. [Google Scholar] [CrossRef]
- Gordon, E. State intervention in pregnancy: Should the law respond thus to the problem of Foetal Alcohol Spectrum Disorder? J. Law Med. 2015, 23, 156–188. [Google Scholar]
- Corrales-Gutierrez, I.; Mendoza, R.; Gomez-Baya, D.; Leon-Larios, F. Pregnant Women’s Risk Perception of the Teratogenic Effects of Alcohol Consumption in Pregnancy. J. Clin. Med. 2019, 8, 907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, N.N.; Burd, L.; Grant, T.; Edwards, W.; Adler, R.; Streissguth, A. Prenatal alcohol exposure: An assessment strategy for the legal context. Int. J. Law Psychiatry 2015, 42–43, 144–148. [Google Scholar] [CrossRef]
- Mcmurtrie, J. The criminal justice system’s disparate treatment of individuals with fetal alcohol spectrum disorders in cases involving sexual activity. J. Psychiatry Law 2011, 39, 159–177. [Google Scholar] [CrossRef]
- Conry, J.; Fast, D. Mental health issues for people with fetal alcohol spectrum disorders in the criminal justice system. Can. J. Community Ment. Health 2010, 29, 65–70. [Google Scholar] [CrossRef]
- Greenmyer, J.R.; Klug, M.G.; Kambeitz, C.; Popova, S.; Burd, L. A multicountry updated assessment of the economic impact of fetal alcohol spectrum disorder: Costs for children and adults. J. Addict. Med. 2018, 12, 466–473. [Google Scholar] [CrossRef]
- Popova, S.; Lange, S.; Burd, L.; Rehm, J. Cost attributable to Fetal Alcohol Spectrum Disorder in the Canadian correctional system. Int. J. Law Psychiatry 2015, 41, 76–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrales-Gutierrez, I.; Mendoza, R.; Gomez-Baya, D.; Leon-Larios, F. Understanding the Relationship between Predictors of Alcohol Consumption in Pregnancy: Towards Effective Prevention of FASD. Int. J. Environ. Res. Public Health 2020, 17, 1388. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Reference | Country | Study | Main Findings |
|---|---|---|---|
| Streissguth et al., 2004 [21] | USA | Sample: 415 subjects including 155 with FAS and 260 with fetal alcohol exposure (FAE) were enrolled: 60% white, 25% Indigenous American, 7% Black, 6% Hispanic. Diagnosis: Diagnoses were by dysmorphologists. Methodology of the study: Life History Interview administered by telephone. Economic status: No data were reported. | Psychological tests in FAS and FAE subjects revealed two main deficits: specific arithmetic disability and specific adaptive behavior problems, evaluating criminal behavior. |
| Cockram, 2005 [22] | Australia | Sample: group of offenders with intellectual disability (843). Aboriginal 8.3%. Diagnosis: not reported. Methodology of the study: Analysis of Disability Services Commission (DSC) database. Economic status: No data were reported. | This study shows that subjects with an intellectual disability received a prison sentence in 11.3% of cases, while offenders without an intellectual disability received a prison sentence in 8.9%. |
| Rojas and Gretton, 2007 [23] | Canada | Sample: Aboriginal (n = 102) and non-Aboriginal (n = 257) youth who engaged in sexual offending behavior and were ordered to attend a sexual offender treatment program were enrolled. FASD subjects (n = 63) Diagnosis: Diagnoses based on database data, analyzing participants’ discharge from a Youth Sexual Offence Treatment Program (YSOTP). Methodology of the study: Analysis of database. Economic status: No data were reported | This study shows that Aboriginal youth were more likely to be affected by FASD, substance abuse, child victimization, academic difficulties and instability in the living environment. Aboriginal youth were significantly more likely than non-Aboriginal youth to have a living situation rated as unstable. |
| Salmon and Buetow, 2012 [24] | New Zealand | Sample: 14 subjects (6 Maori, 6 New Zealanders European, 1 America, 1 Cook Island) with FAS were enrolled. Diagnosis: professionally diagnosed Methodology of the study: interview (audio-recorded, face-to-face in-depth, unstructured questioning was used). Economic status: Concerning their economic status, 6 were not employed, 2 employed, 6 no answer. | All participants reported mental disorders due to the use of alcohol and recreational drugs. Some participants were involved with the justice and/or the legal system. FASD was considered during the judicial phases. |
| Momino et al., 2012 [25] | Brazil | Sample: 262 male adolescents institutionalized because of criminal behavior (alcohol use admitted by 48.8% of the mothers) and 154 male students (alcohol use admitted by 39.9% of the mothers) were enrolled. Diagnosis: FAS diagnostic signs were defined according the guidelines of the Institute of Medicine. Methodology of the study: A questionnaire was completed by the mother or by the legal guardian. Economic status: No data were reported. | The results of this study showed that criminal behavior was more pronounced in the FAS group, although this was influenced by complex environmental and social interactions, including prenatal exposure to alcohol. |
| McLachlan et al., 2014 [26] | Canada | Sample: Two groups of young offenders (50 with FASD and 50 without prenatal alcohol exposure) Diagnosis: professionally diagnosed Methodology of the study: Questionnaire. Economic status: No data were reported. | The findings showed that a large number of young offenders with FASD (90%) demonstrated impairment in at least one psychological skill and the rates of impairment were significantly higher than in the comparison group. |
| Rangmar et al., 2015 [11] | Sweden | Sample: Data of 79 subjects with FAS were compared with Control Group (n = 3160). Diagnosis: Diagnoses were performed based on literature indication. Methodology of the study: Database (national register–based study) analysis. Economic status: About 82% of subjects with FAS had a disposable income in the 3 lowest quintiles. | Analyzing the criminal acts committed in the two groups, 27.8% of the subjects in the FASD group had at least one record of a judicial conviction (20.3% in the control group) and 6.3% had been convicted of a serious crime (4.0% in the control group). |
| Banerji and Shah, 2017 [27] | Canada | Sample: 49 children with FASD were enrolled in this study Diagnosis: The diagnoses of FASD were based on the 2005 Canadian guidelines. Methodology of the study: Interview and database analysis (interviews with the biological mother, review of medical or social service records). Economic status: No data were reported. | Subjects with FASD demonstrated various problems such as learning difficulties and behavioral problems, developmental delay, attention deficit hyperactivity disorder (ADHD), alcohol abuse. Moreover, 6/49 were involved with the criminal justice system. |
| Tait et al., 2017 [28] | Canada | Sample: Two male psychiatric patients with FASD with criminal issues Diagnosis: The diagnoses of FASD were based on the 2005 Canadian guidelines. Methodology of the study: Follow-up during life. Economic status: No data were reported. | The authors underlined the importance of support programs in order to guarantee the long-term stability for individuals living with FASD. |
| Bower et al., 2018 [29] | Australia | Sample: 99 young subjects were included in this study: 88 subjects had at least one domain of severe neurodevelopmental impairment and 36 were diagnosed with FASD; 73 are Aboriginal. Diagnosis: Australian diagnostic criteria were applied. Methodology of the study: Face-to-face approach. Economic status: No data were reported. | This study confirmed that subjects with FASD show severe neurodevelopmental disorders. |
| McLachlan et al., 2018 [30] | Canada | Sample: 100 justice-involved youth were enrolled, including 50 diagnosed with FASD and 50 without FASD or prenatal alcohol exposure. Diagnosis: Not reported. Methodology of the study: Interview and database analysis. Economic status: No data were reported. | The results of this study support the validity of violence risk assessment tools (such as the Structured Assessment of Violence Risk in Youth and the Youth Level of Service/Case Management Inventory) in predicting recidivism in justice-involved young subjects with FASD. |
| McLachlan et al., 2019 [31] | Canada | Sample: 80 justice-involved adults were enrolled. Diagnosis: the 2005 Canadian Diagnostic Guidelines for FASD with the support of FAS facial photographic analysis software. Methodology of the study: Interview, using semi-structured medical and social history interview. Economic status: No data were reported. | In the sample analyzed, the authors identified about 17% of the subjects with FASD; moreover, about 31% of subjects had been exposed to alcohol in the prenatal period. |
| Brintnell et al., 2019 [32] | Canada | Sample: 49 subjects (Caucasian (37%) and Indigenous (57%), with 12% of Indigenous participants identified with specific First, Nation groups and 6% whose ethnicity was unknown) with FADS were recruited. Diagnosis: neuropsychological testing and a psychiatric interview Methodology of the study: Test and Interview. Economic status: No data were reported. | The sample analyzed confirms the finding that FASD is a risk factor for criminal behavior. |
| Flannigan et al., 2019 [33] | Canada | Sample: The authors compared two groups: FASD (38) vs non-FASD (43). Diagnosis: not reported. Methodology of the study: Database revision. Economic status: No data were reported. | Based on numerous parameters analyzed, subjects with FASD displayed a severely impaired neurocognitive functioning profile compared to the control group. |
| Brownell et al., 2019 [34] | Canada | Sample: 1058 subjects with FASD compared with non-FASD (2229) subjects. Diagnosis: Diagnoses based on the reported data. Methodology of the study: Database analysis. Economic status: Nearly two-thirds (63%) of the FASD group was in the lowest income quintile (Q1); about one-third (29%) in the non-FASD group. | The results show that although FASD subjects had similar involvement with health services as non-FASD subjects, they were more likely to be charged with a crime, showing greater involvement with the judiciary. |
| Kambeitz et al., 2019 [35] | USA | Sample: The data of 98 subjects with FASD were compared with data of 105 non-FASD (controls). Diagnosis: Based on different published criteria. Methodology of the study: Database analysis. Economic status: No data were reported. | Data from the present study confirm that subjects with FASD are more likely to have adverse childhood events (ACEs) than the control group. Increased ACEs were associated with higher rates of neurodevelopmental disorders for subjects with FASD. |
| Mela et al., 2020 [36] | Canada | Sample: 45 subjects were included in the study from an outpatient forensic psychiatric clinic. Diagnosis: Canadian guidelines for diagnosing FASD. Methodology of the study: self-report questionnaires. Economic status: The authors reported that: 14% was employed full-time, 11.6% part-time, 7% full-time student, 23.3% sick/disability leave, 41.9% was unemployed, 2.3% retired. | The results of this study showed that subjects in the FASD group committed fewer total offenses than those in the No-FASD group, although no statistically significant differences were reported. However, significant cognitive impairment was found in the FASD group compared to the control group. |
| Mullaly et al., 2020 [37] | Canada | Sample: Data of FASD group (25 subjects with a confirmed or possible FASD diagnosis) were compared with data of the criminal justice (CJ) group (55 subjects without FASD). Diagnosis: 2005 Canadian Diagnostic Guidelines for FASD. Methodology of the study: Tests and data analysis. Economic status: No data were reported. | The main findings of this study showed that participants with diagnosed/possible FASD were more likely to fail a single performance validity test (PVT) and failed more PVTs overall than those without FASD. Participants in the FASD group had an IQ <70 on a standard measure of intellectual functioning compared to the control group. |
| Hamilton et al., 2020 [38] | Australia | Sample: 38 participants were enrolled (27 were aboriginal youths; 9 subjects with confirmed FASD diagnosis). Diagnosis: Not reported. Methodology of the study: Interview (structured, semi-structured and unstructured interviewing). Economic status: No data were reported. | The authors underlined the importance of FASD diagnosis in subjects in prison in order to have a correct trial. |
| Hashmi et al., 2021 [39] | Canada | Sample: 61 cases were included (44% indigenous people), 36% with FASD. Diagnosis: multidisciplinary team. Methodology of the study: Legal database analysis. Economic status: Lower socioeconomic status. | Cognitive impairment may be considered an important risk factor in order to commit a crime, particularly in the cases of sexual violence. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sessa, F.; Salerno, M.; Esposito, M.; Di Nunno, N.; Li Rosi, G.; Roccuzzo, S.; Pomara, C. Understanding the Relationship between Fetal Alcohol Spectrum Disorder (FASD) and Criminal Justice: A Systematic Review. Healthcare 2022, 10, 84. https://doi.org/10.3390/healthcare10010084
Sessa F, Salerno M, Esposito M, Di Nunno N, Li Rosi G, Roccuzzo S, Pomara C. Understanding the Relationship between Fetal Alcohol Spectrum Disorder (FASD) and Criminal Justice: A Systematic Review. Healthcare. 2022; 10(1):84. https://doi.org/10.3390/healthcare10010084
Chicago/Turabian StyleSessa, Francesco, Monica Salerno, Massimiliano Esposito, Nunzio Di Nunno, Giuseppe Li Rosi, Salvatore Roccuzzo, and Cristoforo Pomara. 2022. "Understanding the Relationship between Fetal Alcohol Spectrum Disorder (FASD) and Criminal Justice: A Systematic Review" Healthcare 10, no. 1: 84. https://doi.org/10.3390/healthcare10010084