
The Effectiveness of Smoking Cessation, Alcohol Reduction, Diet and Physical Activity Interventions in Improving Maternal and Infant Health Outcomes: A Systematic Review of Meta-Analyses

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
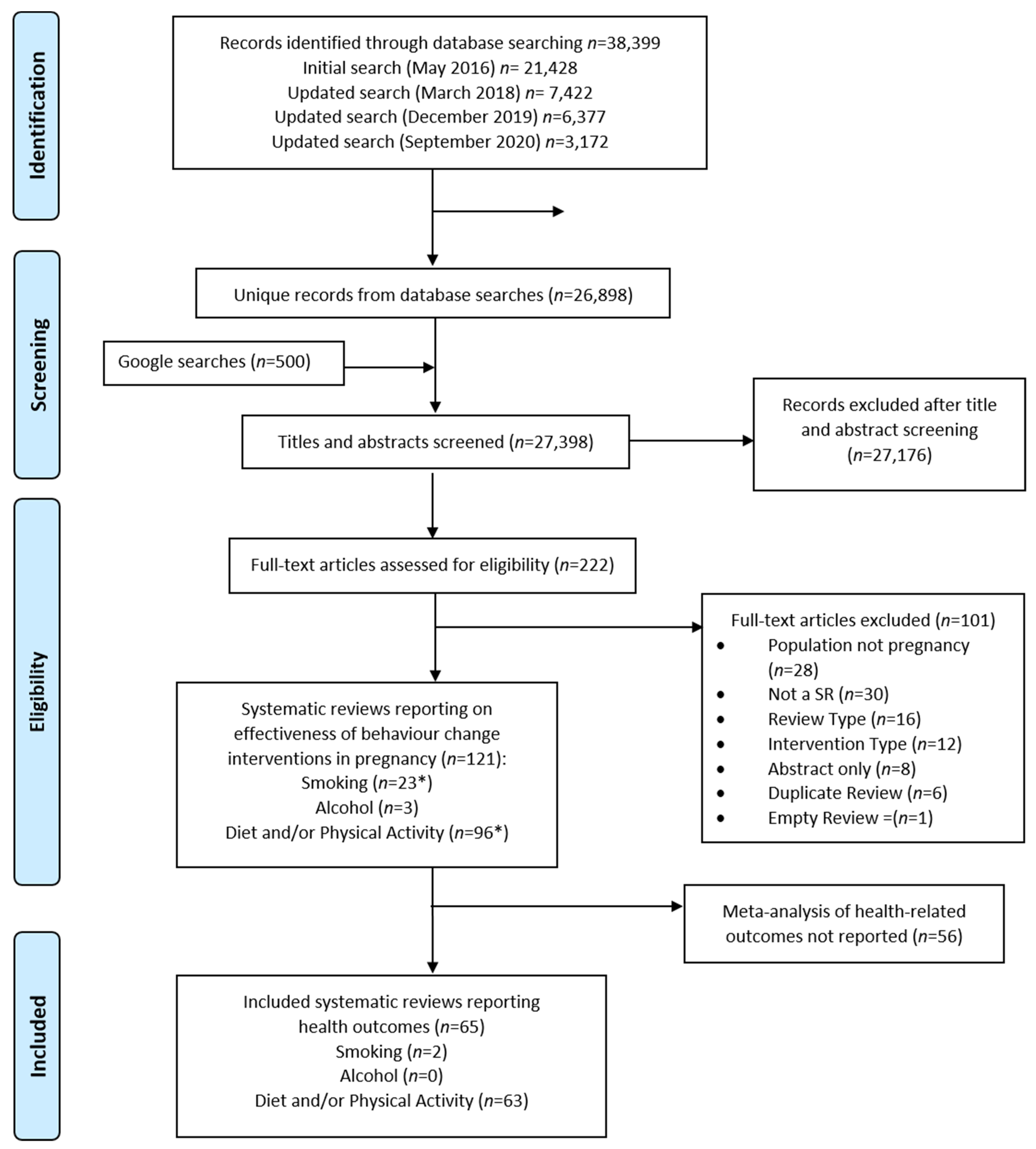
2.1. Identification of Studies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Evidence Synthesis
3. Results
3.1. Included Systematic Reviews
3.1.1. Quality
3.1.2. Overlap of Included Studies
3.2. Maternal Health Outcomes
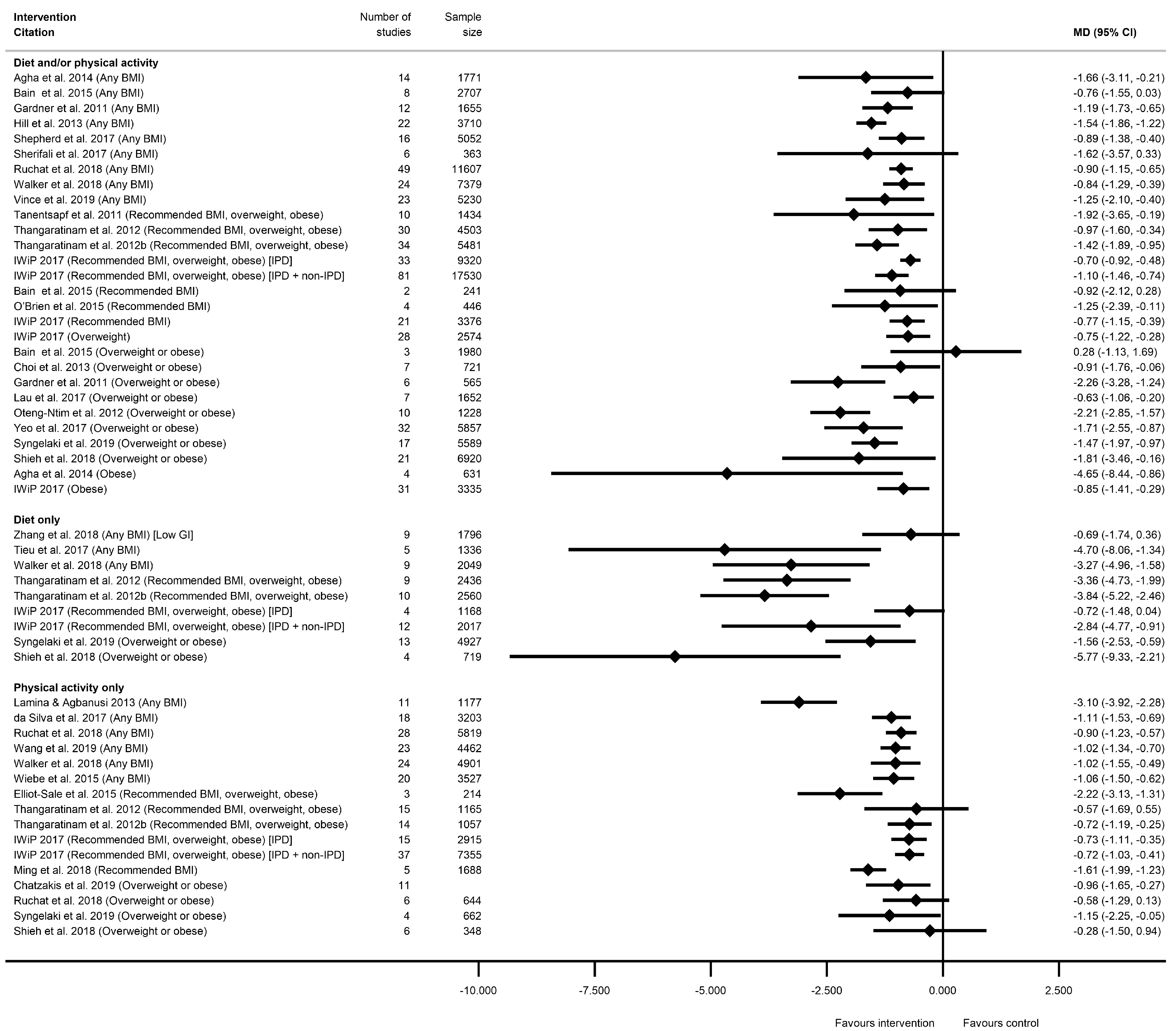
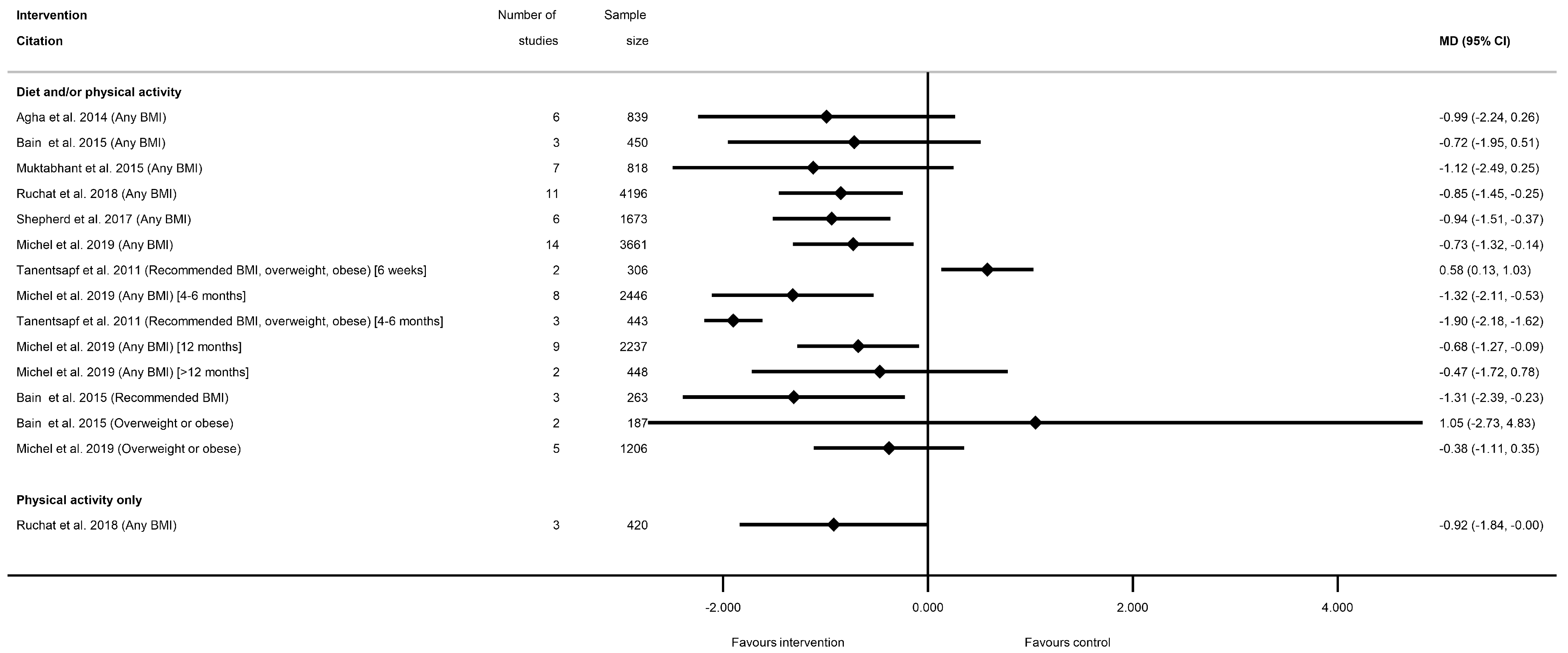
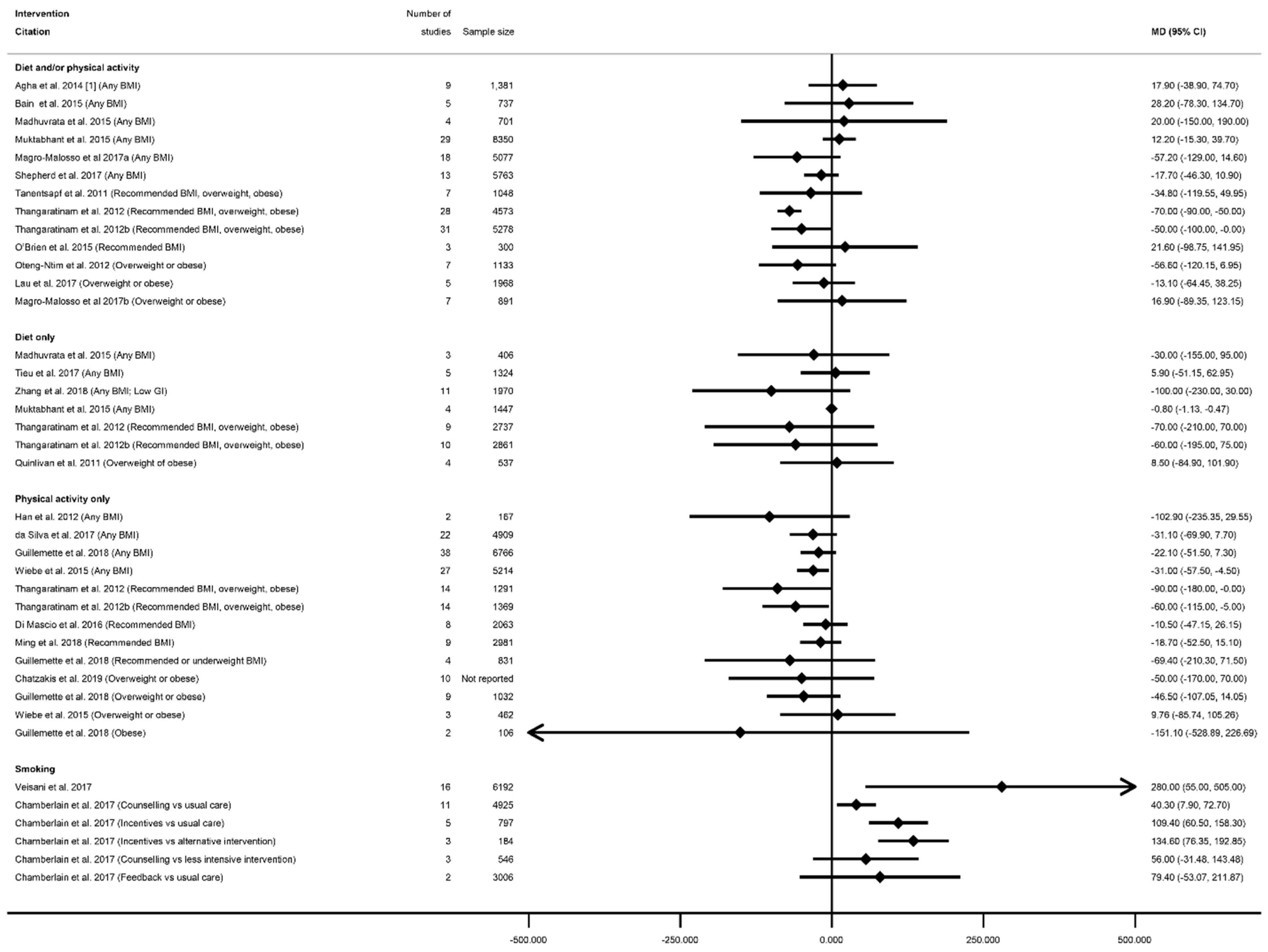
3.2.1. Maternal Weight-Related Outcomes
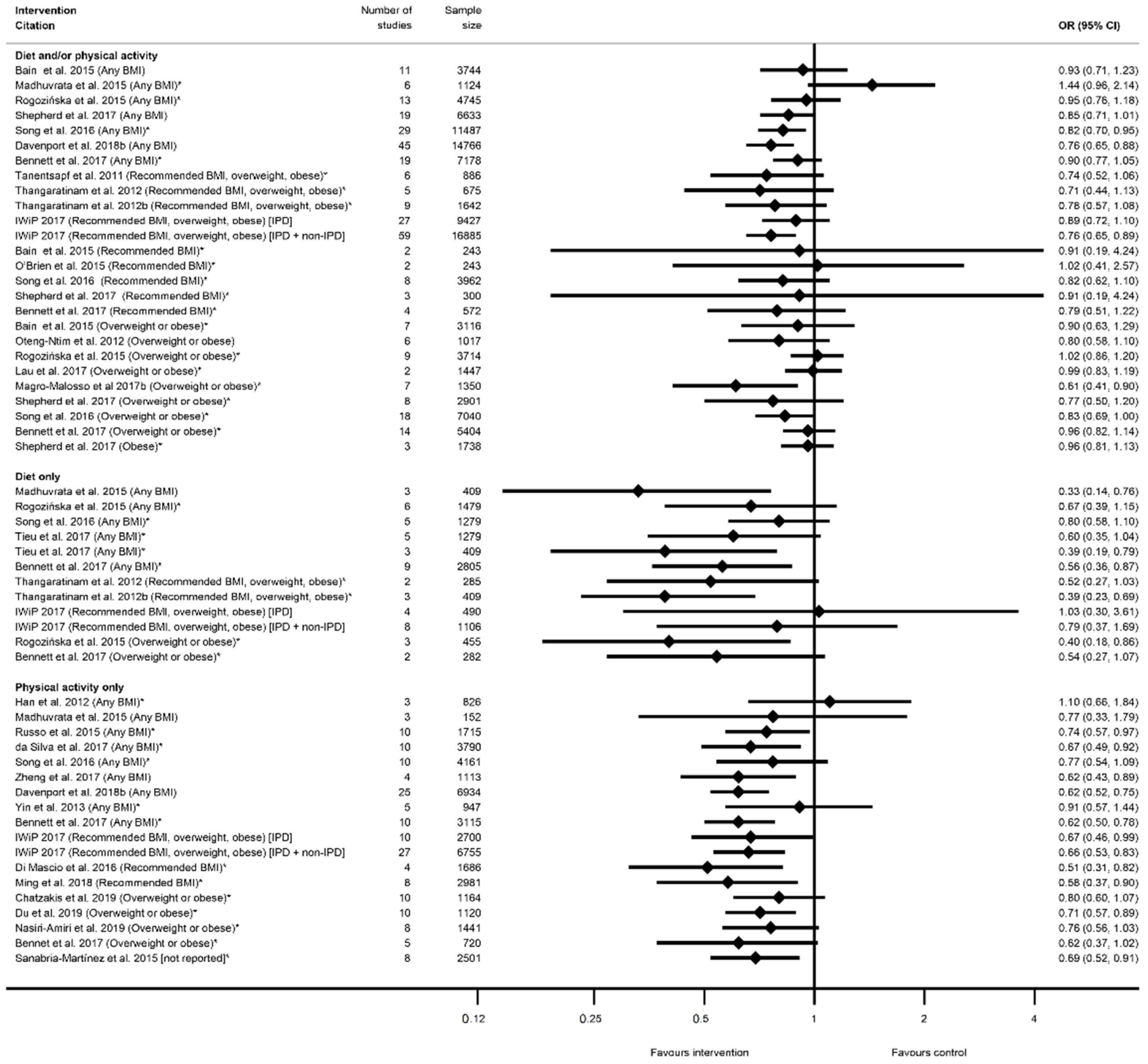
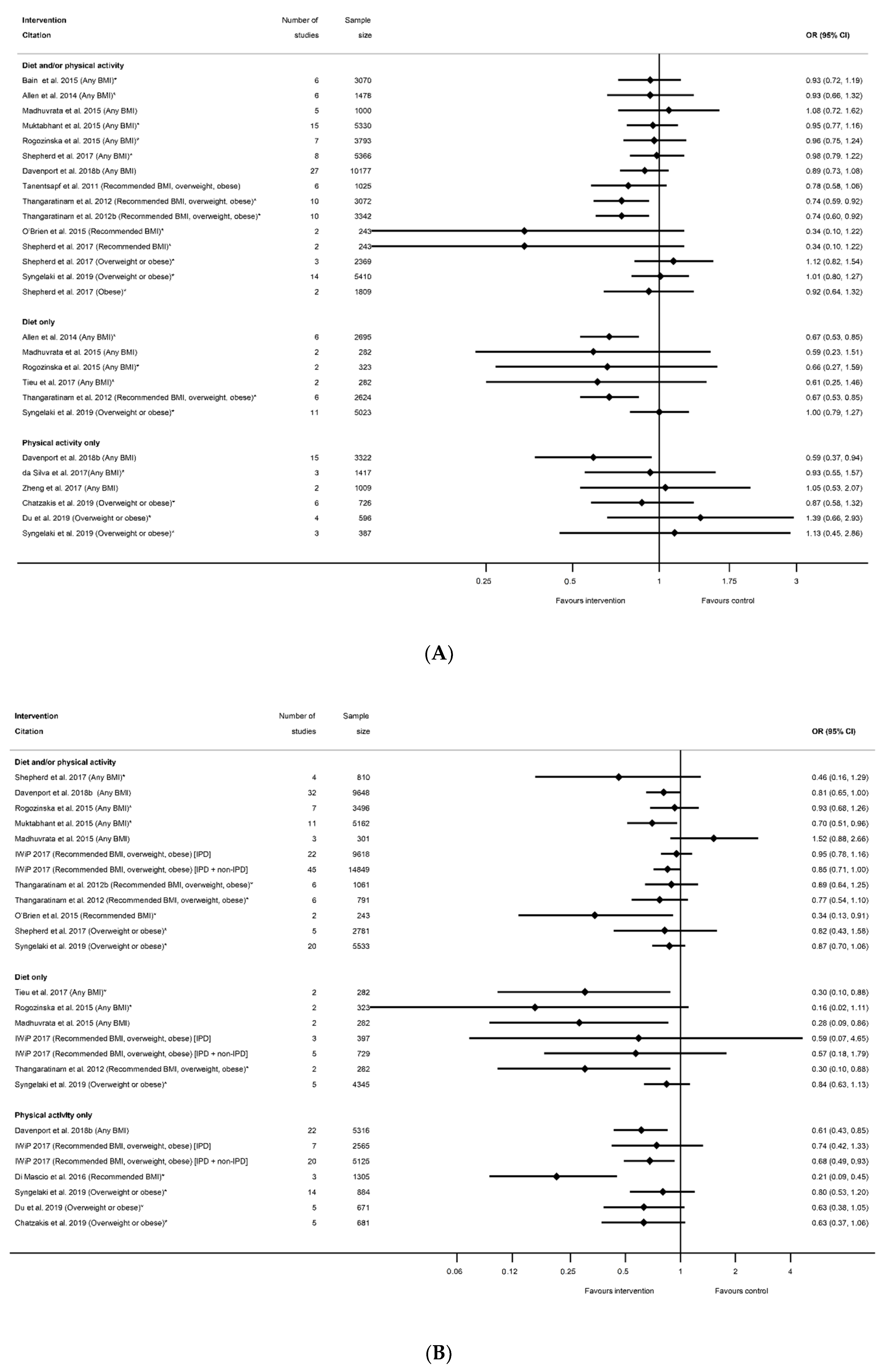
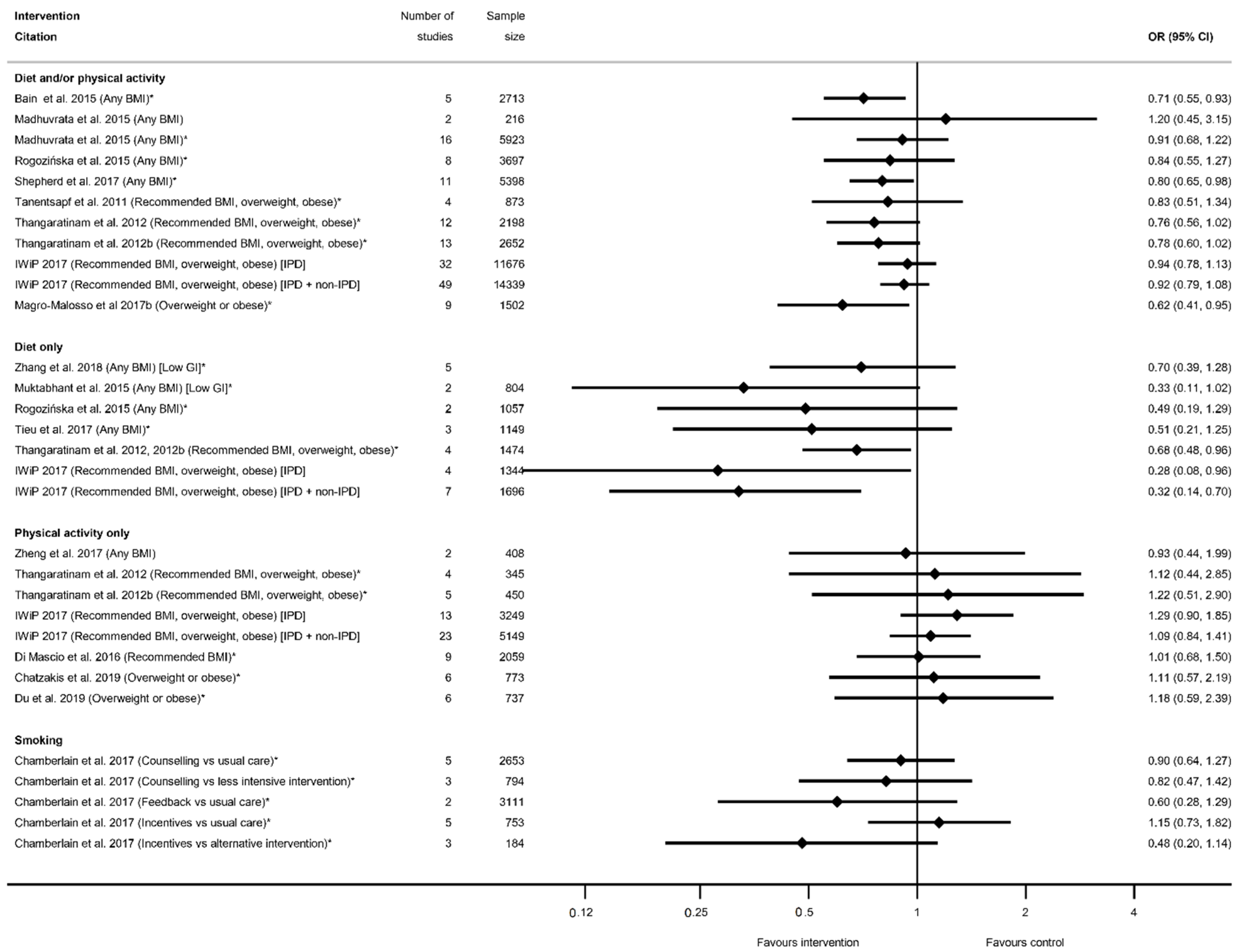
3.2.2. Gestational Diabetes Related Outcomes
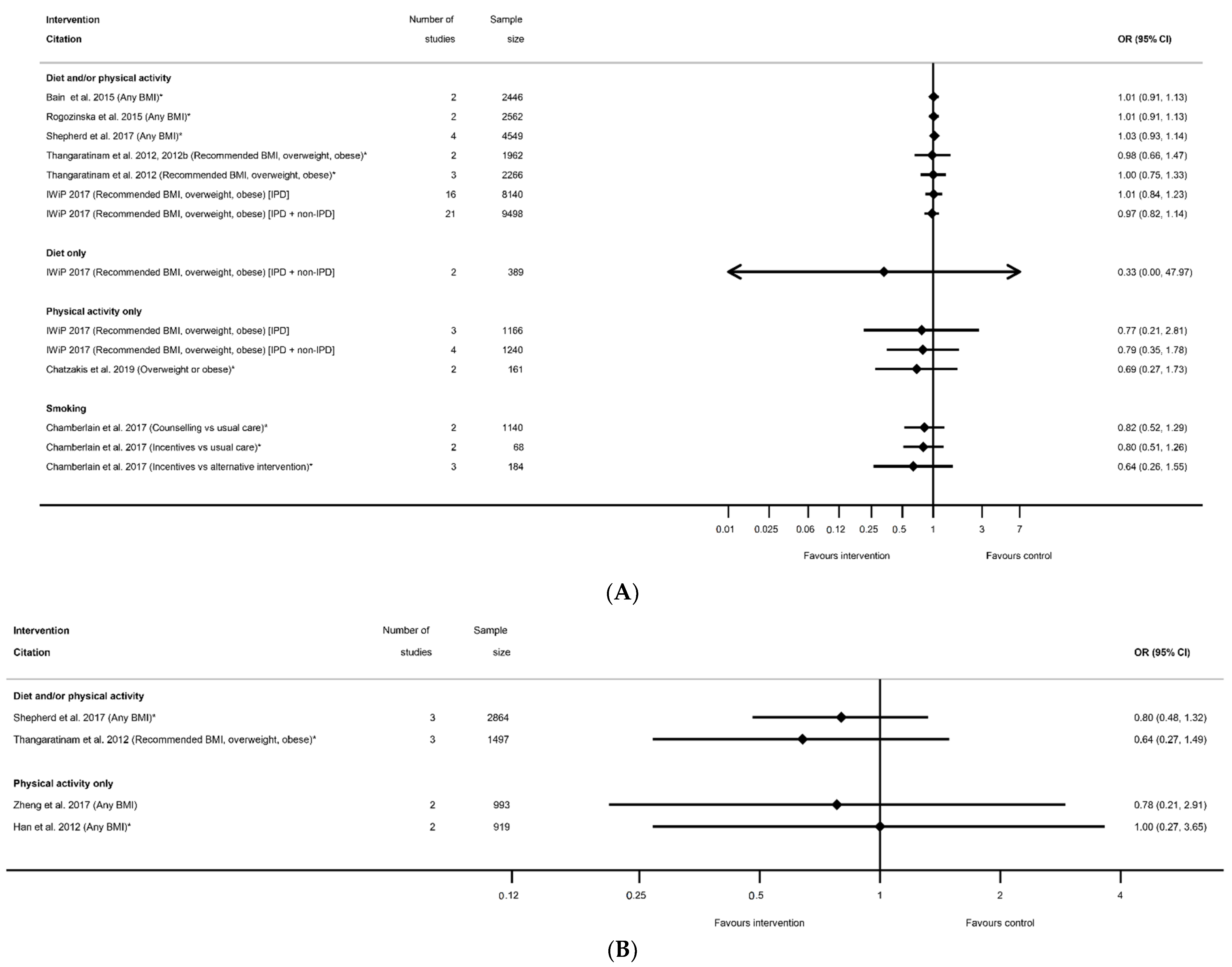
3.2.3. Hypertensive Disorders
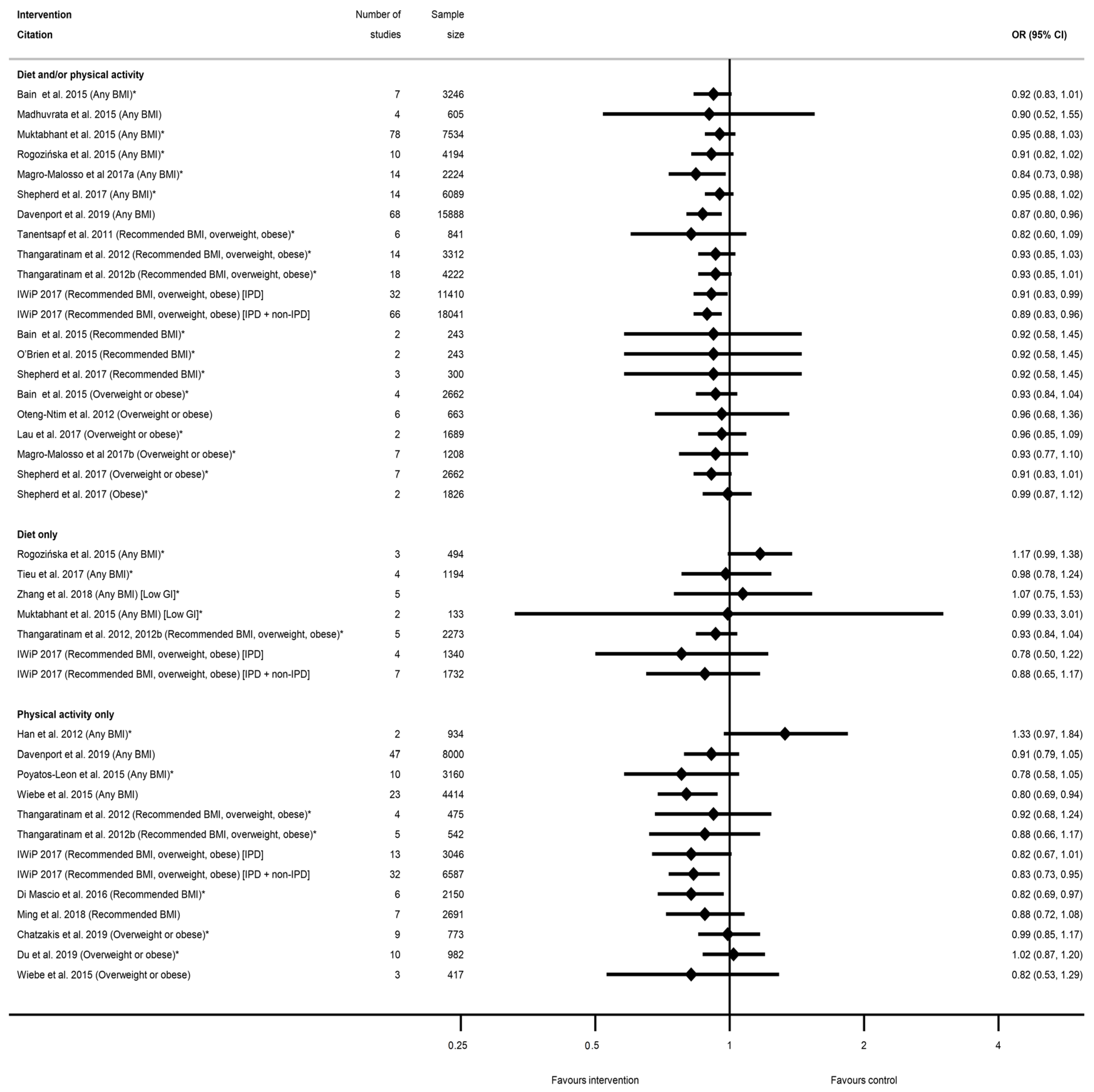
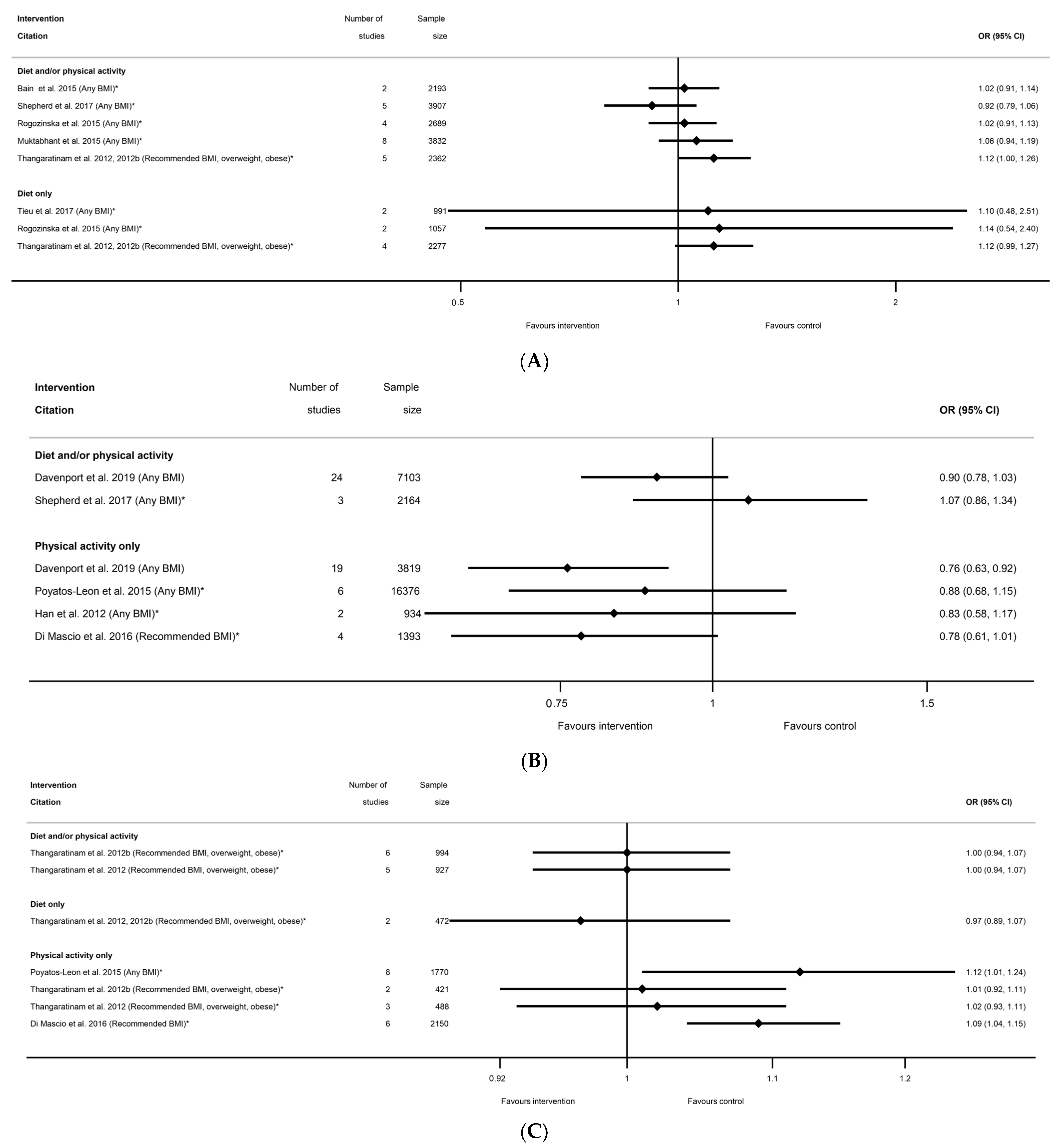
3.2.4. Mode of Delivery Outcomes
3.2.5. Other Maternal Health Outcomes
3.3. Infant Health Outcomes
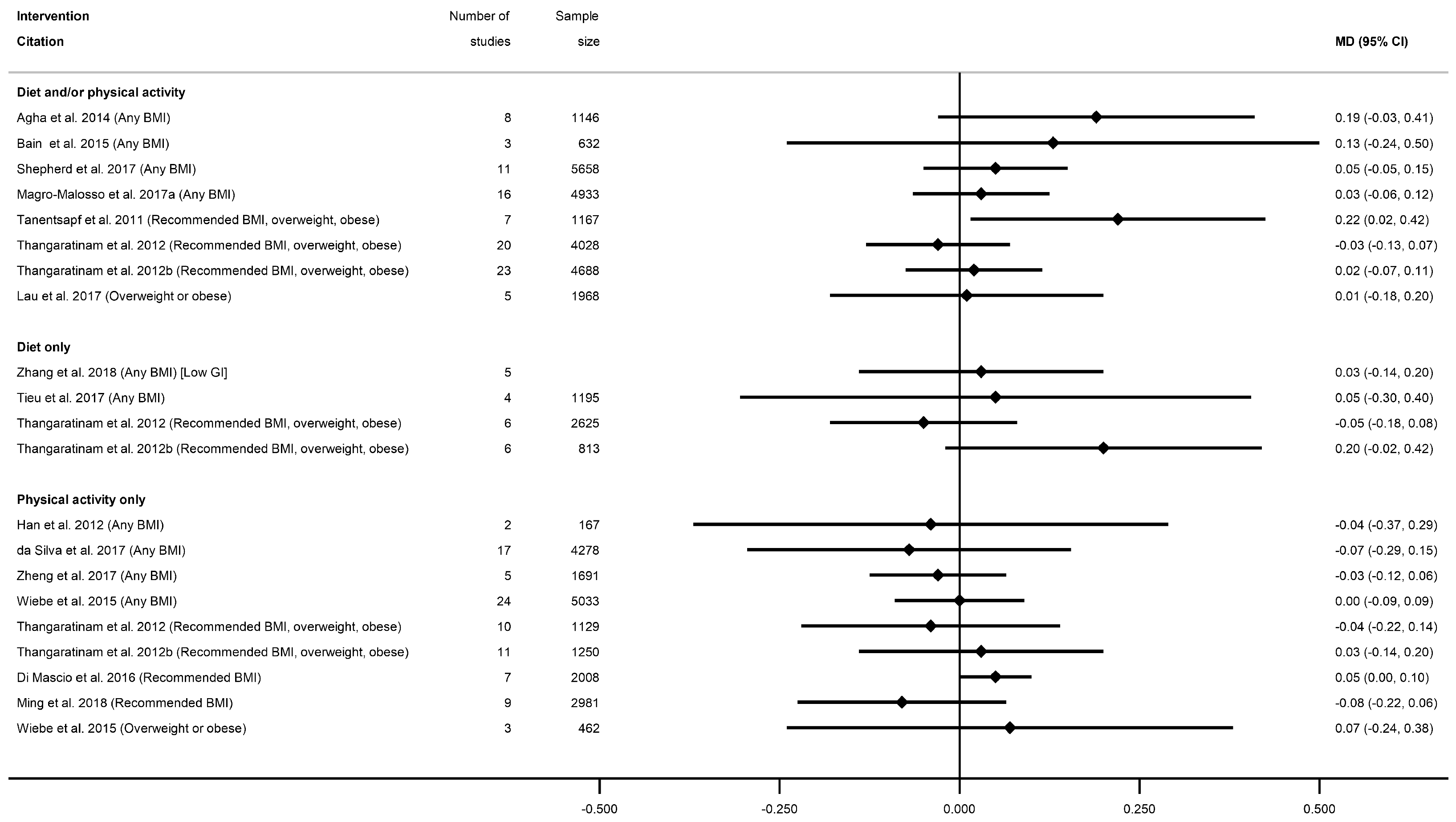
3.3.1. Fetal Growth Outcomes
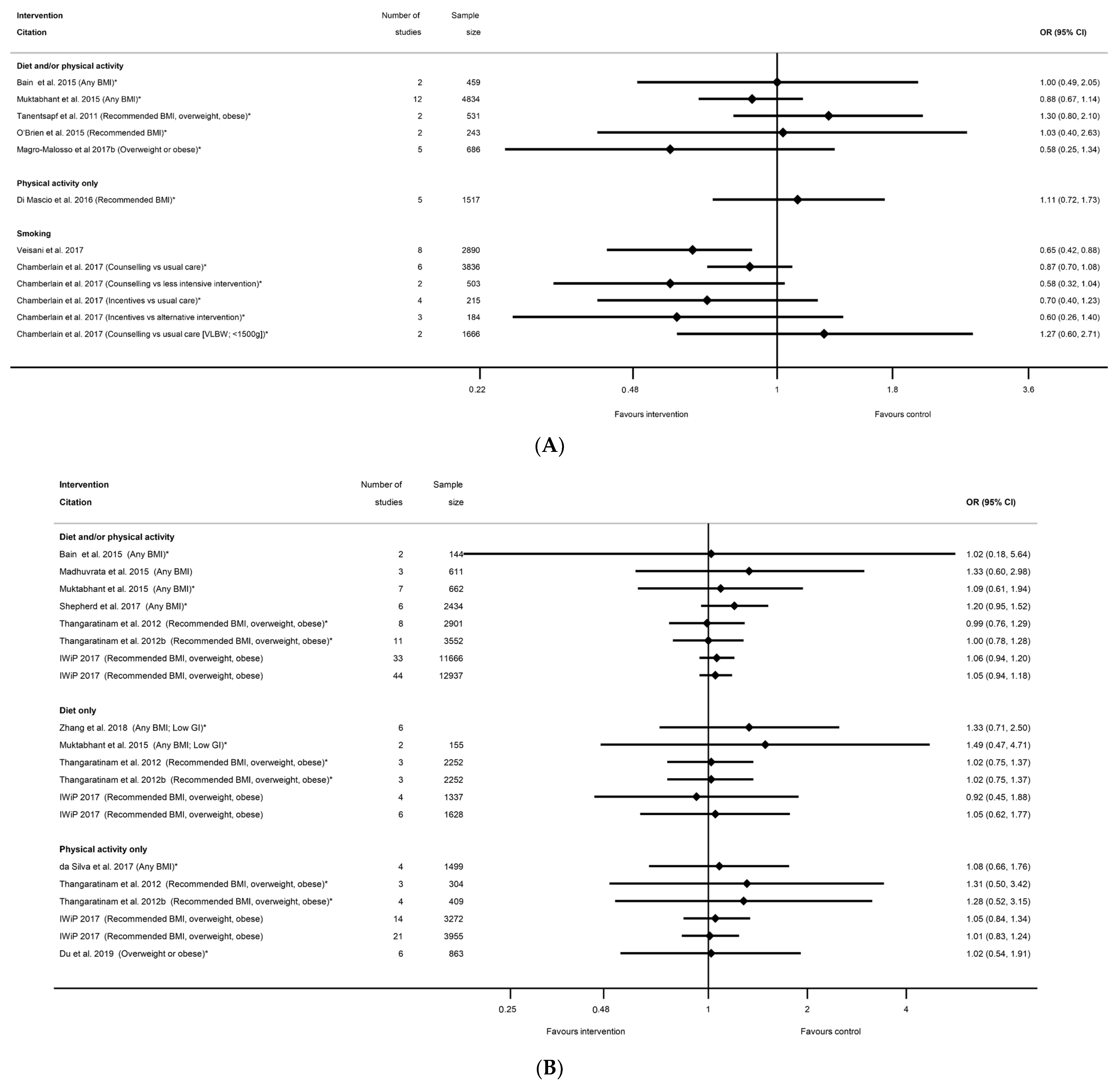
3.3.2. Gestational Age at Delivery Outcomes
3.3.3. Mortality Outcomes
3.3.4. Neonatal Intensive Care Unit Admission
3.3.5. Apgar Score
3.3.6. Other Infant Health-Related Outcomes
3.4. Conflict of Interest
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pineles, B.L.; Park, E.; Samet, J.M. Systematic Review and Meta-Analysis of Miscarriage and Maternal Exposure to Tobacco Smoke during Pregnancy. Am. J. Epidemiol. 2014, 179, 807–823. [Google Scholar] [CrossRef] [Green Version]
- Pineles, B.L.; Hsu, S.; Park, E.; Samet, J.M. Systematic Review and Meta-Analyses of Perinatal Death and Maternal Exposure to Tobacco Smoke during Pregnancy. Am. J. Epidemiol. 2016, 184, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, P.P.d.S.; Da Mata, F.A.F.; Figueiredo, A.C.G.; de Andrade, K.R.C.; Pereira, M.G. Maternal Active Smoking During Pregnancy and Low Birth Weight in the Americas: A Systematic Review and Meta-analysis. Nicotine Tob. Res. 2017, 19, 497–505. [Google Scholar] [CrossRef]
- Liu, B.; Xu, G.; Sun, Y.; Qiu, X.; Ryckman, K.K.; Yu, Y.; Snetselaar, L.G.; Bao, W. Maternal cigarette smoking before and during pregnancy and the risk of preterm birth: A dose–response analysis of 25 million mother–infant pairs. PLoS Med. 2020, 17, e1003158. [Google Scholar] [CrossRef] [PubMed]
- Mamluk, L.; Edwards, H.B.; Savović, J.; Leach, V.; Jones, T.; Moore, T.H.M.; Ijaz, S.; Lewis, S.J.; Donovan, J.L.; Lawlor, D.; et al. Low alcohol consumption and pregnancy and childhood outcomes: Time to change guidelines indicating apparently ‘safe’ levels of alcohol during pregnancy? A systematic review and meta-analyses. BMJ Open 2017, 7, e015410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marufu, T.C.; Ahankari, A.; Coleman, T.; Lewis, S. Maternal smoking and the risk of still birth: Systematic review and meta-analysis. BMC Public Health 2015, 15, 239. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Saugstad, O.D.; Henriksen, T.; Tonstad, S. Maternal Body Mass Index and the Risk of Fetal Death, Stillbirth, and Infant Death: A Systematic Review and Meta-analysis. JAMA 2014, 311, 1536–1546. [Google Scholar] [CrossRef] [Green Version]
- Slack, E.; Best, K.E.; Rankin, J.; Heslehurst, N. Maternal obesity classes, preterm and post-term birth: A retrospective analysis of 479,864 births in England. BMC Pregnancy Childbirth 2019, 19, 434. [Google Scholar] [CrossRef]
- Skagerstrom, J.; Chang, G.; Nilsen, P. Predictors of drinking during pregnancy: A systematic review. J. Women’s Health 2011, 20, 901–913. [Google Scholar] [CrossRef] [Green Version]
- Nykjaer, C.; Alwan, N.A.; Greenwood, D.C.; Simpson, N.A.B.; Hay, A.W.M.; White, K.L.M.; Cade, J.E. Maternal alcohol intake prior to and during pregnancy and risk of adverse birth outcomes: Evidence from a British cohort. J. Epidemiol. Community Health 2014, 68, 542–549. [Google Scholar] [CrossRef] [Green Version]
- Elliott, L.; Coleman, K.; Suebwongpat, A.; Norris, S. Fetal Alcohol Spectrum Disorders (FASD): Systematic reviews of prevention, diagnosis and management. In Health Services Assessment Collaboration Report; National Institute for Health Research: Auckland, New Zealand, 2008; Volume 1. [Google Scholar]
- Najafi, F.; Hasani, J.; Izadi, N.; Hashemi-Nazari, S.; Namvar, Z.; Mohammadi, S.; Sadeghi, M. The effect of prepregnancy body mass index on the risk of gestational diabetes mellitus: A systematic review and dose-response meta-analysis. Obes. Rev. 2019, 20, 472–486. [Google Scholar] [CrossRef]
- De Seymour, J.; Chia, A.; Colega, M.; Jones, B.; McKenzie, E.; Shirong, C.; Godfrey, K.; Kwek, K.; Saw, S.-M.; Conlon, C.; et al. Maternal Dietary Patterns and Gestational Diabetes Mellitus in a Multi-Ethnic Asian Cohort: The GUSTO Study. Nutrients 2016, 8, 574. [Google Scholar] [CrossRef]
- Pham, N.M.; Do, V.V.; Lee, A.H. Polyphenol-rich foods and risk of gestational diabetes: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2019, 73, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Cheung, N.W. Associations of Diet and Physical Activity with Risk for Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 698. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. Towards a Smokefree Generation: A Tobacco Control Plan for England; Do, H., Ed.; Department of Health: London, UK, 2017. [Google Scholar]
- National Institute for Health and Care Excellence. Public Health Guidelines [PH27]: Weight Management before, during and after Pregnancy; NICE: London, UK, 2010. [Google Scholar]
- National Institute for Health and Care Excellence. NICE Guidelines PH26: Quitting Smoking in Pregnancy and Following Childbirth; NICE: London, UK, 2010. [Google Scholar]
- Alavi, N.; Haley, S.; Chow, K.; McDonald, S.D. Comparison of national gestational weight gain guidelines and energy intake recommendations. Obes. Rev. 2013, 14, 68–85. [Google Scholar] [CrossRef] [PubMed]
- UK Chief Medical Officers. Low Risk Drinking Guidelines; UK Chief Medical Officers: London, UK, 2016. [Google Scholar]
- O’Leary, C.M.H.L.; Elliott, E.J.; Bower, C. A review of policies on alcohol use during pregnancy in Australia and other English-speaking countries, 2006. Med. J. Aust. 2007, 186, 466–471. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. NICE Guidelines CG62: Antenatal Care; NICE: London, UK, 2008. [Google Scholar]
- Heslehurst, N.; Hayes, L.; Jones, D.; Newham, J.; Olajide, J.; McLeman, L.; McParlin, C.; De Brun, C.; Azevedo, L. The effectiveness of smoking cessation, alcohol reduction, diet and physical activity interventions in changing behaviours during pregnancy: A systematic review of systematic reviews. PLoS ONE 2020, 15, e0232774. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute. The Joanna Briggs Institute Reviewers’ Manual 2014: Methodology for JBI Umbrella Reviews; The Joanna Briggs Institute: Adelaide, Australia, 2014. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinsdale, S.; Azevedo, L.B.; Shucksmith, J.; Newham, J.; Ells, L.J.; Jones, D.; Heslehurst, N. Effectiveness of weight management, smoking cessation and alcohol reduction interventions in changing behaviors during pregnancy: An umbrella review protocol. BI Database Syst. Rev. Implement. Rep. 2016, 14, 29–47. [Google Scholar] [CrossRef] [Green Version]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A product from the ESRC Methods Programme; Lancaster University: Lancaster, UK, 2006. [Google Scholar]
- Agha, M.; Agha, R.A.; Sandall, J. Interventions to reduce and prevent obesity in pre-conceptual and pregnant women: A systematic review and meta-analysis. PLoS ONE 2014, 9, e95132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bain, E.; Crane, M.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2015, Cd010443, Epub 2015/04/13. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.; Rogozinska, E.; Sivarajasingam, P.; Khan, K.S.; Thangaratinam, S. Effect of diet- and lifestyle-based metabolic risk-modifying interventions on preeclampsia: A meta-analysis. Acta Obstet. Gynecol. Scand. 2014, 93, 973–985. [Google Scholar] [CrossRef] [PubMed]
- Campbell, F.; Johnson, M.; Messina, J.; Guillaume, L.; Goyder, E. Behavioural interventions for weight management in pregnancy: A systematic review of quantitative and qualitative data. BMC Public Health 2011, 11, 491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.; Fukuoka, Y.; Lee, J.H. The effects of physical activity and physical activity plus diet interventions on body weight in overweight or obese women who are pregnant or in postpartum: A systematic review and meta-analysis of randomized controlled trials. Prev. Med. 2013, 56, 351–364. [Google Scholar] [CrossRef] [Green Version]
- Elliott-Sale, K.J.; Barnett, C.T.; Sale, C. Exercise interventions for weight management during pregnancy and up to 1 year postpartum among normal weight, overweight and obese women: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Gardner, B.; Wardle, J.; Poston, L.; Croker, H. Changing diet and physical activity to reduce gestational weight gain: A meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2011, 12, e602–e620. [Google Scholar] [CrossRef] [PubMed]
- Gresham, E.; Bisquera, A.; Byles, J.E.; Hure, A.J. Effects of dietary interventions on pregnancy outcomes: A systematic review and meta-analysis. Matern. Child Nutr. 2016, 12, 5–23. [Google Scholar] [CrossRef]
- Han, S.; Middleton, P.; Crowther, C.A. Exercise for pregnant women for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2012, Cd009021. [Google Scholar] [CrossRef]
- Hill, B.; Skouteris, H.; Fuller-Tyszkiewicz, M. Interventions designed to limit gestational weight gain: A systematic review of theory and meta-analysis of intervention components. Obes. Rev. 2013, 14, 435–450. [Google Scholar] [CrossRef]
- Lamina, S.; Agbanusi, E. Effect of aerobic exercise training on maternal weight gain in pregnancy: A meta-analysis of randomized controlled trials. Ethiop. J. Health Sci. 2013, 23, 59–64. [Google Scholar]
- Madhuvrata, P.; Govinden, G.; Bustani, R.; Song, S.; Farrell, T.A. Prevention of gestational diabetes in pregnant women with risk factors for gestational diabetes: A systematic review and meta-analysis of randomised trials. Obs. Med. 2015, 8, 68–85. [Google Scholar] [CrossRef] [Green Version]
- Muktabhant, B.; Lawrie, T.A.; Lumbiganon, P.; Laopaiboon, M. Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst. Rev. 2015, Cd007145. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, C.M.; Grivell, R.M.; Dodd, J.M. Systematic review of antenatal dietary and lifestyle interventions in women with a normal body mass index. Acta Obs. Gynecol. Scand. 2016, 95, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Oostdam, N.; van Poppel, M.N.; Wouters, M.G.; van Mechelen, W. Interventions for preventing gestational diabetes mellitus: A systematic review and meta-analysis. J. Women’s Health 2011, 20, 1551–1563. [Google Scholar] [CrossRef]
- Oteng-Ntim, E.; Varma, R.; Croker, H.; Poston, L.; Doyle, P. Lifestyle interventions for overweight and obese pregnant women to improve pregnancy outcome: Systematic review and meta-analysis. BMC Med. 2012, 10, 47. [Google Scholar] [CrossRef] [Green Version]
- Quinlivan, J.A.; Julania, S.; Lam, L. Antenatal dietary interventions in obese pregnant women to restrict gestational weight gain to Institute of Medicine recommendations: A meta-analysis. Obs. Gynecol. 2011, 118, 1395–1401. [Google Scholar] [CrossRef] [PubMed]
- Rogozińska, E.; Chamillard, M.; Hitman, G.A.; Khan, K.S.; Thangaratinam, S. Nutritional manipulation for the primary prevention of gestational diabetes mellitus: A meta-analysis of randomised studies. PLoS ONE 2015, 10, e0115526. [Google Scholar] [CrossRef] [Green Version]
- Russo, L.M.; Nobles, C.; Ertel, K.A.; Chasan-Taber, L.; Whitcomb, B.W. Physical activity interventions in pregnancy and risk of gestational diabetes mellitus: A systematic review and meta-analysis. Obs. Gynecol. 2015, 125, 576–582. [Google Scholar] [CrossRef]
- Sanabria-Martínez, G.; García-Hermoso, A.; Poyatos-León, R.; Álvarez-Bueno, C.; Sánchez-López, M.; Martínez-Vizcaíno, V. Effectiveness of physical activity interventions on preventing gestational diabetes mellitus and excessive maternal weight gain: A meta-analysis. Bjog Int. J. Obstet. Gynaecol. 2015, 122, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Streuling, I.; Beyerlein, A.; Rosenfeld, E.; Hofmann, H.; Schulz, T.; von Kries, R. Physical activity and gestational weight gain: A meta-analysis of intervention trials. Bjog Int. J. Obstet. Gynaecol. 2011, 118, 278–284. [Google Scholar] [CrossRef]
- Sui, Z.; Grivell, R.M.; Dodd, J.M. Antenatal exercise to improve outcomes in overweight or obese women: A systematic review. Acta Obs. Gynecol. Scand. 2012, 91, 538–545. [Google Scholar] [CrossRef]
- Tanentsapf, I.; Heitmann, B.L.; Adegboye, A.R.A. Systematic review of clinical trials on dietary interventions to prevent excessive weight gain during pregnancy among normal weight, overweight and obese women. BMC Pregnancy Childbirth 2011, 11, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thangaratinam, S.; Rogozińska, E.; Jolly, K.; Glinkowski, S.; Duda, W.; Borowiack, E.; Roseboom, T.; Tomlinson, J.; Walczak, J.; Kunz, R.; et al. Interventions to reduce or prevent obesity in pregnant women: A systematic review. Health Technol. Assess. 2012, 16, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thangaratinam, S.; Rogozinska, E.; Jolly, K.; Glinkowski, S.; Roseboom, T.J.; Tomlinson, J.W.; Kunz, R.; Mol, B.W.; Coomarasamy, A.; Khan, K.S. Effects of interventions in pregnancy on maternal weight and obstetric outcomes: Meta-analysis of randomised evidence. BMJ Br. Med. J. 2012, 344, e2088. [Google Scholar] [CrossRef] [Green Version]
- da Silva, S.G.; Ricardo, L.I.; Evenson, K.R.; Hallal, P.C. Leisure-Time Physical Activity in Pregnancy and Maternal-Child Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Cohort Studies. Sports Med. 2017, 47, 295–317. [Google Scholar] [CrossRef]
- Di Mascio, D.; Magro-Malosso, E.R.; Saccone, G.; Marhefka, G.D.; Berghella, V. Exercise during pregnancy in normal-weight women and risk of preterm birth: A systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 2016, 215, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Weight Management in Pregnancy (IWiP) collaboration. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: Meta-analysis of individual participant data from randomised trials. BMJ (Clin. Res. Ed.) 2017, 358, j3119. [Google Scholar] [CrossRef] [Green Version]
- Lau, Y.; Klainin-Yobas, P.; Htun, T.P.; Wong, S.N.; Tan, K.L.; Ho-Lim, S.T. Electronic-based lifestyle interventions in overweight or obese perinatal women: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 1071–1087. [Google Scholar] [CrossRef]
- Magro-Malosso, E.R.; Saccone, G.; Di Tommaso, M.; Roman, A.; Berghella, V. Exercise during pregnancy and risk of gestational hypertensive disorders: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2017, 96, 921–931. [Google Scholar] [CrossRef] [Green Version]
- Magro-Malosso, E.R.; Saccone, G.; Di Mascio, D.; Di Tommaso, M.; Berghella, V. Exercise during pregnancy and risk of preterm birth in overweight and obese women: A systematic review and meta-analysis of randomized controlled trials. Acta Obs. Gynecol. Scand. 2017, 96, 263–273. [Google Scholar] [CrossRef] [Green Version]
- Sanabria-Martínez, G.; García-Hermoso, A.; Poyatos-León, R.; González-García, A.; Sánchez-López, M.; Martínez-Vizcaíno, V. Effects of Exercise-Based Interventions on Neonatal Outcomes: A Meta-Analysis of Randomized Controlled Trials. Am. J. Health Promot. 2016, 30, 214–223. [Google Scholar] [CrossRef]
- Shepherd, E.; Gomersall, J.C.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 11, Cd010443. [Google Scholar] [CrossRef]
- Sherifali, D.; Nerenberg, K.A.; Wilson, S.; Semeniuk, K.; Ali, M.U.; Redman, L.M. The Effectiveness of eHealth Technologies on Weight Management in Pregnant and Postpartum Women: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2017, 19, e337. [Google Scholar] [CrossRef]
- Song, C.; Li, J.; Leng, J.; Ma, R.C.; Yang, X. Lifestyle intervention can reduce the risk of gestational diabetes: A meta-analysis of randomized controlled trials. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2016, 17, 960–969. [Google Scholar] [CrossRef]
- Tieu, J.; Shepherd, E.; Middleton, P.; Crowther, C.A. Dietary advice interventions in pregnancy for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 1, Cd006674. [Google Scholar] [CrossRef]
- Yeo, S.; Walker, J.S.; Caughey, M.C.; Ferraro, A.M.; Asafu-Adjei, J.K. What characteristics of nutrition and physical activity interventions are key to effectively reducing weight gain in obese or overweight pregnant women? A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Han, S.; Chen, G.-C.; Li, Z.-N.; Silva-Zolezzi, I.; Parés, G.V.; Wang, Y.; Qin, L.-Q. Effects of low-glycemic-index diets in pregnancy on maternal and newborn outcomes in pregnant women: A meta-analysis of randomized controlled trials. Eur. J. Nutr. 2018, 57, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Wang, H.; Ren, M. Influence of exercise intervention on gestational diabetes mellitus: A systematic review and meta-analysis. J. Endocrinol. Investig. 2017, 40, 1027–1033. [Google Scholar] [CrossRef]
- Gresham, E.; Byles, J.E.; Bisquera, A.; Hure, A.J. Effects of dietary interventions on neonatal and infant outcomes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 1298–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatzakis, C.; Goulis, D.G.; Mareti, E.; Eleftheriades, M.; Zavlanos, A.; Dinas, K. Prevention of gestational diabetes mellitus in overweight or obese pregnant women: A network meta-analysis. Diabetes Res. Clin. Pr. 2019, 158, 107924. [Google Scholar] [CrossRef] [PubMed]
- Craemer, K.A.; Sampene, E.; Safdar, N.; Antony, K.M.; Wautlet, C.K. Nutrition and Exercise Strategies to Prevent Excessive Pregnancy Weight Gain: A Meta-analysis. Am. J. Perinatol. Rep. 2019, 9, e92–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davenport, M.H.; Kathol, A.J.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J. Prenatal exercise is not associated with fetal mortality: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; McCurdy, A.P.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Riske, L.; et al. Impact of prenatal exercise on both prenatal and postnatal anxiety and depressive symptoms: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1376. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.J.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Ruchat, S.-M.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Impact of prenatal exercise on maternal harms, labour and delivery outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Sobierajski, F.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Gray, C.E.; Garcia, A.J.; Barrowman, N.; Riske, L.; et al. Glucose responses to acute and chronic exercise during pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1357–1366. [Google Scholar] [CrossRef]
- Du, M.C.; Ouyang, Y.Q.; Nie, X.F.; Huang, Y.; Redding, S.R. Effects of physical exercise during pregnancy on maternal and infant outcomes in overweight and obese pregnant women: A meta-analysis. Birth 2019, 46, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Guillemette, L.; Hay, J.L.; Kehler, D.S.; Hamm, N.C.; Oldfield, C.; McGavock, J.M.; Duhamel, T.A. Exercise in Pregnancy and Children’s Cardiometabolic Risk Factors: A Systematic Review and Meta-Analysis. Sports Med. Open 2018, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Michel, S.; Raab, R.; Drabsch, T.; Günther, J.; Stecher, L.; Hauner, H. Do lifestyle interventions during pregnancy have the potential to reduce long-term postpartum weight retention? A systematic review and meta-analysis. Obes. Rev. 2019, 20, 527–542. [Google Scholar] [CrossRef]
- Ming, W.-K.; Ding, W.; Zhang, C.J.P.; Zhong, L.; Long, Y.; Li, Z.; Sun, C.; Wu, Y.; Chen, H.; Chen, H.; et al. The effect of exercise during pregnancy on gestational diabetes mellitus in normal-weight women: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2018, 18, 440. [Google Scholar] [CrossRef] [Green Version]
- Morison, P.N.; Bacardi-Gascon, M.; Lopez-Corrales, M.; Jimenez-Cruz, A. Combined dietary-exercise intervention for gestational weight gain and birthweight: A meta-analysis. Asia Pac. J. Clin. Nutr. 2018, 27, 860–868. [Google Scholar] [CrossRef]
- Nasiri-Amiri, F.; Sepidarkish, M.; Shirvani, M.A.; Habibipour, P.; Tabari, N.S.M. The effect of exercise on the prevention of gestational diabetes in obese and overweight pregnant women: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 72. [Google Scholar] [CrossRef] [Green Version]
- Ruchat, S.-M.; Mottola, M.F.; Skow, R.J.; Nagpal, T.S.; Meah, V.L.; James, M.; Riske, L.; Sobierajski, F.; Kathol, A.J.; Marchand, A.-A.; et al. Effectiveness of exercise interventions in the prevention of excessive gestational weight gain and postpartum weight retention: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1347. [Google Scholar] [CrossRef]
- Syngelaki, A.; Sequeira Campos, M.; Roberge, S.; Andrade, W.; Nicolaides, K.H. Diet and exercise for preeclampsia prevention in overweight and obese pregnant women: Systematic review and meta-analysis. Br. J. Sports Med. 2019, 32, 3495–3501. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wen, D.; Liu, X.; Liu, Y. Impact of exercise on maternal gestational weight gain: An updated meta-analysis of randomized controlled trials. Medicine 2019, 98, e16199. [Google Scholar] [CrossRef] [PubMed]
- Poyatos-León, R.; García-Hermoso, A.; Sanabria-Martínez, G.; Álvarez-Bueno, C.; Sánchez-López, M.; Martínez-Vizcaíno, V. Effects of exercise during pregnancy on mode of delivery: A meta-analysis. Acta Obs. Gynecol. Scand. 2015, 94, 1039–1047. [Google Scholar] [CrossRef]
- Walker, R.; Bennett, C.; Blumfield, M.; Gwini, S.; Ma, J.; Wang, F.; Wan, Y.; Truby, H. Attenuating Pregnancy Weight Gain-What Works and Why: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincze, L.; Rollo, M.; Hutchesson, M.; Hauck, Y.; MacDonald-Wicks, L.; Wood, L.; Callister, R.; Collins, C. Interventions including a nutrition component aimed at managing gestational weight gain or postpartum weight retention: A systematic review and meta-analysis. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 297–364. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, H.W.; Boulé, N.G.; Chari, R.; Davenport, M.H. The Effect of Supervised Prenatal Exercise on Fetal Growth: A Meta-analysis. Obstet. Gynecol. 2015, 125, 1185–1194. [Google Scholar] [CrossRef]
- Yin, Y.N.; Li, X.L.; Tao, T.J.; Luo, B.R.; Liao, S.J. Physical activity during pregnancy and the risk of gestational diabetes mellitus: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2014, 48, 290–295. [Google Scholar] [CrossRef]
- Shieh, C.; Cullen, D.L.; Pike, C.; Pressler, S.J. Intervention strategies for preventing excessive gestational weight gain: Systematic review and meta-analysis. Obes. Rev. 2018, 19, 1093–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, C.J.; Walker, R.E.; Blumfield, M.L.; Gwini, S.-M.; Ma, J.; Wang, F.; Wan, Y.; Dickinson, H.; Truby, H. Interventions designed to reduce excessive gestational weight gain can reduce the incidence of gestational diabetes mellitus: A systematic review and meta-analysis of randomised controlled trials. Diabetes Res. Clin. Pract. 2018, 141, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, C.; O’Meara-Eaves, A.; Porter, J.; Coleman, T.; Perlen, S.M.; Thomas, J.; McKenzie, J.E. Psychosocial interventions for supporting women to stop smoking in pregnancy. Cochrane Database Syst. Rev. 2017, 2, Cd001055. [Google Scholar] [CrossRef]
- Veisani, Y.; Jenabi, E.; Delpisheh, A.; Khazaei, S. Effect of prenatal smoking cessation interventions on birth weight: Meta-analysis. J. Matern. Neonatal Med. 2019, 32, 332–338. [Google Scholar] [CrossRef] [PubMed]
- World Bank. World Bank Country and Lending Groups 2019. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 17 October 2019).
- World Health Organization. World Health Statistics 2018. Available online: www.who.int/gho/publications/world_health_statistics/2018/en:2018 (accessed on 22 March 2021).
- Branca, F.; Lartey, A.; Oenema, S.; Aguayo, V.; Stordalen, G.A.; Richardson, R. Transforming the food system to fight non-communicable diseases. BMJ (Clin. Res. Ed.) 2019, 364, l296. [Google Scholar] [CrossRef] [Green Version]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Systematic Reviews Reporting Smoking Interventions (n = 2) | Systematic Reviews Reporting Diet and/or Physical Activity Interventions (n = 37) | Systematic Reviews Reporting Diet-only Interventions (n = 19) | Systematic Reviews Reporting Physical-Activity-only Interventions (n = 37) | |
|---|---|---|---|---|
| Time period of included intervention studies in the reviews | ||||
| Range in years: | 1976 to 2016 | 1974 to 2018 | 1975 to 2018 | 1974 to 2019 |
| Search strategies: | ||||
| Databases only (n) | 0 | 3 | 1 | 2 |
| Supplementary searches (n) | 2 | 34 | 18 | 35 |
| Included study designs: | ||||
| RCT only (n) | 2 | 24 | 18 | 27 |
| RCT + other design (n) | 0 | 13 | 1 | 10 |
| Number included studies in the systematic reviews | ||||
| Range (n) | 16 to 88 | 5 to 113 | 4 to 89 | 3 to 113 |
| Median (n) | N/A | 21 (IQR 14 to 46) | 23 (IQR 14 to 44) | 23 (IQR 10 to 49) |
| Pooled sample sizes included in the systematic reviews | ||||
| Range (n women) | 6192 to >26,000 | 363 to 273,182 | 537 to 182,139 | 214 to 598,185 |
| Median (n women) | N/A | 6920 (IQR 2748 to 12,007) | 8558 (IQR 2786 to 11,487) | 4350 (IQR 1768 to 14,601) |
| Not reported (n) | 1 * | 0 | 0 | 1 * |
| Countries of intervention studies included in the systematic reviews (reported for n systematic reviews) | Not reported for 6 systematic reviews | Not reported for 6 systematic reviews | Not reported for 7 systematic reviews | |
| HICs represented in the included interventions | 1. Australia 2. Canada 3. Denmark 4. France 5. Greece 6. Ireland 7. Netherlands 8. New Zealand 9. Norway 10. Poland 11. Spain 12. Sweden 13. UK 14. USA | 1. Australia 2. Belgium 3. Canada 4. Croatia 5. Denmark 6. Finland 7. France 8. Germany 9. Greece 10. Ireland 11. Italy 12. Japan 13. Netherlands 14. New Zealand 15. Norway 16. Poland 17. Portugal 18. South Korea 19. Spain 20. Sweden 21. Switzerland 22. Taiwan 23. UK 24. USA | 1. Australia 2. Belgium 3. Canada 4. Chile 5. Denmark 6. Finland 7. Germany 8. Greece 9. Ireland 10. Italy 11. Netherlands 12. New Zealand 13. Norway 14. Spain 15. Sweden 16. Taiwan 17. UK 18. USA | 1. Australia 2. Belgium 3. Canada 4. Croatia 5. Denmark 6. Finland 7. France 8. Germany 9. Greece 10. Ireland 11. Italy 12. Japan 13. Netherlands 14. New Zealand 15. Norway 16. Poland 17. Portugal 18. South Korea 19. Spain 20. Sweden 21. Switzerland 22. Taiwan 23. UK 24. USA |
| UMICs represented in the included interventions | 1. Argentina 2. Brazil 3. Columbia 4. Cuba 5. Mexico | 1. Argentina 2. Brazil 3. China 4. Colombia 5. Iran 6. Kosovo 7. Mexico 8. Serbia 9. South Africa 10. Thailand 11. Turkey | 1. Argentina 2. Brazil 3. China 4. Columbia 5. Indonesia (East Java) 6. Iran 7. Kosovo 8. Mexico 9. South Africa 10. Turkey | 1. Argentina 2. Brazil 3. China 4. Colombia 5. Iran 6. Kosovo 7. Mexico 8. Serbia 9. South Africa 10. Thailand 11. Turkey |
| LMICs represented in the included interventions | None | 1. Benin 2. Egypt 3. India 4. Pakistan | 1. Egypt 2. India | 1. Benin 2. Egypt 3. India 4. Pakistan |
| LICs represented in the included interventions | None | None | 1. Gambia | None |
| Intervention Type | Quality Assessment Question | Total Score | Quality Category | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Smoking interventions | 100% (2/2) | 100% (2/2) | 100% (2/2) | 100% (2/2) | 50% (1/2) | 0% (0/2) | 100% (2/2) | 100% (2/2) | 100% (2/2) | 50% (1/2) | 50% (1/2) | Range 7–10 | 50% moderate (1/2) 50% high (1/2) |
| Diet and physical activity interventions | 100% (37/37) | 84% (31/37) | 92% (34/37) | 76% (28/37) | 95% (35/37) | 76% (28/37) | 86% (32/37) | 100% (37/37) | 71% (26/37) | 86% (32/37) | 84% (31/37) | Range 6–11 | 8% moderate (3/37) 92% high (34/37) |
| Diet-only interventions | 100% (19/19) | 74% (14/19) | 89% (17/19) | 79% (15/19) | 89% (17/19) | 79% (15/19) | 84% (16/19) | 100% (19/19) | 89% (17/19) | 89% (17/19) | 89% (17/19) | Range 6–11 | 16% moderate (3/19) 84% high (16/19) |
| Physical-activity-only interventions | 100% (37/37) | 81% (30/37) | 95% (35/37) | 84% (31/37) | 89% (33/37) | 59% (22/37) | 81% (30/37) | 100% (37/37) | 70% (26/37) | 78% (29/37) | 78% (29/37) | Range 6–11 | 14% moderate (5/37) 86% high (32/37) |
| Total for all intervention types * | 100% (65/65) | 86% (56/65) | 94% (61/65) | 85% (55/65) | 89% (58/65) | 69% (45/65) | 85% (55/65) | 100% (65/65) | 72% (47/65) | 85% (55/65) | 78% (51/65) | Range 6–11 | 12% moderate (8/65) 88% high (57/65) |
| Categories of Maternal Outcomes | Systematic Reviews Reporting Meta-Analysis | Number of Meta-Analyses Reported | Smoking Interventions (Outcomes Reported; Number of Meta-Analyses) | Diet and/or Physical Activity Interventions (Outcomes Reported; Number of Meta-Analyses) | Diet-Only Interventions (Outcomes Reported; Number of Meta-Analyses) | Physical-Activity-Only Interventions (Outcomes Reported; Number of Meta-Analyses) |
|---|---|---|---|---|---|---|
| Maternal weight-related outcomes (Table S8) | 38 | 114 | None reported | Total GWG; 32 Weekly GWG; 4 Excess GWG; 9 Inadequate GWG; 5 Adequate GWG; 3 Postnatal weight retention; 15 Other related outcomes; 4 | Total GWG; 10Excess GWG; 1 | Total GWG; 24Excess GWG; 2Inadequate GWG; 2Adequate GWG; 2Postnatal weight retention; 1 |
| GDM-related outcomes (Table S9) | 32 | 73 | None reported | GDM diagnosis; 2 6Other related outcomes; 2 | GDM diagnosis; 14 Other related outcomes; 6 | GDM diagnosis; 19 Other related outcomes; 6 |
| Hypertensive disorders of pregnancy-related outcomes ( Table S10) | 22 | 59 | None reported | Pre-eclampsia; 15 Hypertension; 12 Other related outcomes; 3 | Pre-eclampsia; 6 Hypertension; 8 Other related outcomes; 2 | Pre-eclampsia; 6 Hypertension; 7 |
| Mode of delivery-related outcomes (Table S11) | 25 | 63 | None reported | Caesarean delivery; 21 Induction of labour; 5 Instrumental delivery; 2 Vaginal delivery; 2 | Caesarean delivery; 8 Induction of labour; 3 Vaginal delivery; 1 | Caesarean delivery; 13 Instrumental delivery; 4 Vaginal delivery; 4 |
| Other maternal outcomes (Table S12) | 8 | 23 | None reported | PPH; 3Composite outcome; 1 Low back pain; 1 Perineal trauma; 1 Prenatal mental health; 5 Postnatal mental health; 3 | PPH; 1 Composite outcome; 1 | Composite outcome; 1 Prenatal mental health; 4 Postnatal mental health; 2 |
| Total | 58 systematic reviews * | 334 meta-analyses | 0 meta-analyses | 176 meta-analyses | 61 meta-analyses | 97 meta-analyses |
| Categories of Infant Outcomes | Systematic Reviews Reporting Meta-Analysis | Number of Meta-Analyses Reported | Smoking Interventions (Outcomes Reported; Number of Meta-Analyses) | Diet and/or Physical Activity Interventions (Outcomes Reported; Number of Meta-Analyses) | Diet-Only Interventions (Outcomes Reported; Number of Meta-Analyses) | Physical-Activity-Only Interventions (Outcomes Reported; Number of Meta-Analyses) |
|---|---|---|---|---|---|---|
| Fetal growth-related outcomes ( Table S13) | 33 | 150 | Birth weight; 6 Low birth weight; 6 | Birth weight; 14 LGA; 13Macrosomia; 9 SGA; 8 Low birth weight; 5 Other fetal growth; 10 | Birth weight; 9 LGA; 8Macrosomia; 4 SGA; 7 Low birth weight; 1 Other fetal growth; 10 | Birth weight; 16 LGA; 8Macrosomia; 3 SGA; 6 Low birth weight; 1 Other fetal growth; 6 |
| Gestational age at delivery-related outcomes ( Table S14) | 26 | 55 | Preterm; 5 | Gestational age; 8 Preterm; 11 | Gestational age; 5 Preterm; 8 | Gestational age; 10 Preterm; 8 |
| Mortality-related outcomes ( Table S15) | 10 | 17 | Stillbirth; 2 Neonatal mortality; 1 | Stillbirth; 4 Intrauterine death; 1 Neonatal mortality; 1 Perinatal mortality; 2 Miscarriage; 1 | Stillbirth; 1 Perinatal mortality; 1 | Intrauterine death; 1 Perinatal mortality; 1 Miscarriage; 1 |
| NICU ( Table S16) | 7 | 14 | Admission; 3 | Admission; 7 | Admission; 1 | Admission; 3 |
| Apgar score ( Table S17) | 7 | 11 | None reported | <7 at 5 minutes; 2 Score at 1 minute; 1 Score at 5 minutes; 2 | <7 at 5 minutes; 1 Score at 5 minutes; 1 | <7 at 5 minutes; 2 Score at 1 minute; 1 Score at 5 minutes; 1 |
| Other infant health-related outcomes ( Table S18) | 8 | 23 | None reported | Shoulder dystocia; 4 Hypoglycaemia; 3 Respiratory distress; 3 Infant hyperbilirubinemia; 2 Birth trauma; 2 PROM; 1 Breastfeeding; 2 Composite outcome; 1 | Shoulder dystocia; 1 Hypoglycaemia; 1 Placental weight; 1 Composite outcome; 1 | Composite outcome; 1 |
| Total | 36 * | 270 | 23 | 117 | 61 | 69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayes, L.; McParlin, C.; Azevedo, L.B.; Jones, D.; Newham, J.; Olajide, J.; McCleman, L.; Heslehurst, N. The Effectiveness of Smoking Cessation, Alcohol Reduction, Diet and Physical Activity Interventions in Improving Maternal and Infant Health Outcomes: A Systematic Review of Meta-Analyses. Nutrients 2021, 13, 1036. https://doi.org/10.3390/nu13031036
Hayes L, McParlin C, Azevedo LB, Jones D, Newham J, Olajide J, McCleman L, Heslehurst N. The Effectiveness of Smoking Cessation, Alcohol Reduction, Diet and Physical Activity Interventions in Improving Maternal and Infant Health Outcomes: A Systematic Review of Meta-Analyses. Nutrients. 2021; 13(3):1036. https://doi.org/10.3390/nu13031036
Chicago/Turabian StyleHayes, Louise, Catherine McParlin, Liane B Azevedo, Dan Jones, James Newham, Joan Olajide, Louise McCleman, and Nicola Heslehurst. 2021. "The Effectiveness of Smoking Cessation, Alcohol Reduction, Diet and Physical Activity Interventions in Improving Maternal and Infant Health Outcomes: A Systematic Review of Meta-Analyses" Nutrients 13, no. 3: 1036. https://doi.org/10.3390/nu13031036