
Adult Daughters of Alcoholic Parents—A Qualitative Study of These Women’s Pregnancy Experiences and the Potential Implications for Antenatal Care Provision

{kind=link}
Abstract
:1. Introduction
Antenatal Care in Denmark
2. Materials and Methods
2.1. Recruitment and Collection of Data
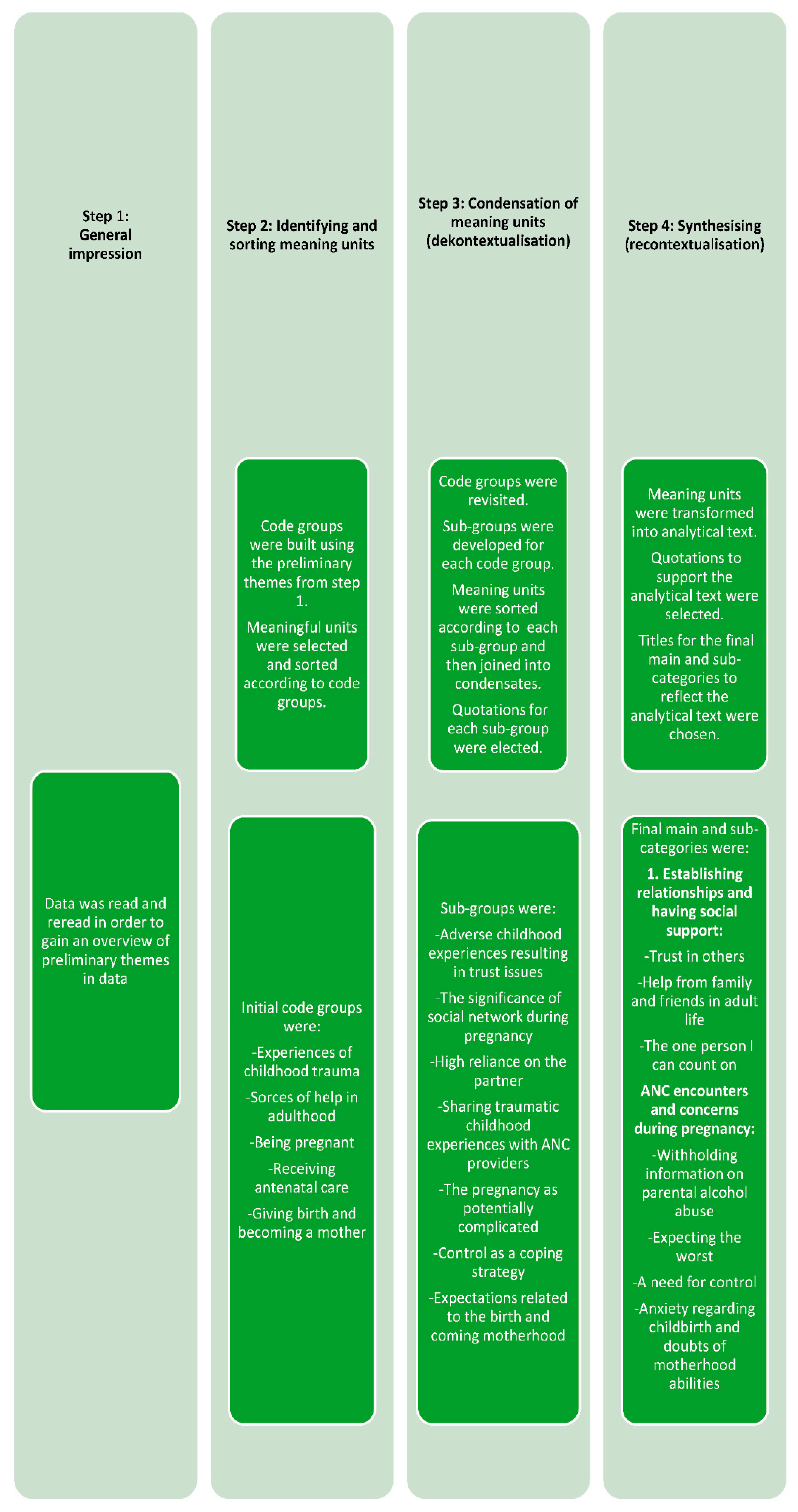
2.2. Data Analysis
2.3. Ethical Considerations
3. Results
3.1. Establishing Relationships and Having Social Support
3.1.1. Trust in Others
“It has affected me a lot. I have always kept people at a distance … even friends I have had since my childhood … I have never allowed myself to feel 100% sure about anyone …”(Pregnant woman, interview 1)
“… I can see how my behaviour is affected by my upbringing… being afraid of being rejected by my husband, anyone, my friends … they probably don’t want to be with me … I won’t contact them … It’s insecurity in myself … am I good enough? … will people like me?”(Pregnant woman, interview 11)
3.1.2. Help from Family and Friends in Adult Life
“… I have never been very social. I have always been somewhat socially handicapped … if you feel something is wrong with you at home, you feel the same in other relationships. I have never been very good at having many relationships and friends … I have very few friends and prefer someone I can trust …”(Pregnant woman, interview 8)
“I am probably not as well balanced as other people … I am very black-and-white, so to speak, if you have plans together, you stick to them … If people don’t follow through on their plans with me … I won’t put up with it … I quickly cut people off if they don’t keep their promises …”(Pregnant woman, interview 6)
3.1.3. The One Person I Can Count On
“… the most important person is without a doubt my boyfriend! He has put up with a lot … (he) is definitely the person who knows me the best and the best support I have now.”(Pregnant woman, interview 9)
“… I talk to my husband a lot (about the pregnancy) … He has the capability to encompass all situations (concerning the pregnancy) … I can see they (my pregnancy concerns) tend to be silly. I am so blessed I have him. He is very down-to-earth and doesn’t worry so much.”(Pregnant woman, interview 8)
“… he tells me: ’It’s good you tell me, I want you to tell me if you are worried’. So, I have used him a lot. He tries to calm me.”(Pregnant woman, interview 10)
3.2. ANC Encounters and Concerns during Pregnancy
3.2.1. Withholding Information on Parental Alcohol Abuse
“… It’s kind of stereotype … connected to the stigma, being the child of an alcoholic … what other people think about this. I have been very private about it. A lot of people don’t know. I need to be very close to a person before I have the courage to tell them … Some are very open about it … I think it is very embarrassing, even though it is not my fault … I don’t want people to judge me because of it.”(Pregnant woman, interview 5)
“I talked to my boyfriend about it. Odd they didn’t ask me about this … In fact, they haven’t talked about it (my upbringing) at any point during my ANC visits.”(Pregnant woman, interview 10)
“… it is written in my antenatal record that I am psychologically vulnerable… My doctor wrote it in case anything turns up … it’s nice that it is recorded in my record.”(Pregnant woman, interview 8)
“… I haven’t talked to my midwife (about how I feel) … I have only seen her twice … The last visit regarded breastfeeding … this did not reflect my needs … breastfeeding is a long time away … There is not a lot of time during the antenatal visits. It is very much like in and out (of the door).”(Pregnant woman, interview 6)
3.2.2. Expecting the Worst
“I am very aware of my food situation… that I get enough to eat and that she (the baby) gets enough … It’s something I can feel preoccupies me a lot.”(Pregnant woman, interview 2)
“… I am by nature or as a result of everything (my childhood experiences) very much a catastrophe thinker. I think of all the things that can go wrong … a month ago … I had a tendency to have high blood pressure … it was very uncomfortable because, as expected, something was wrong and my catastrophe thoughts started rolling.”(Pregnant woman, interview 9)
“… I think … I bring bad fortune. If something can go wrong, it probably will … first I had to get through the ultrasound examinations … then all the worries began.”(Pregnant woman, Interview 11)
“I have catastrophe thoughts … It is something I have to battle … Everything will go wrong … it’s not very nice (to feel like that).”(Pregnant woman, interview 12)
3.2.3. A Need for Control
“I have an enormous need for control … because of my father’s problem (his drinking) … I need things done my way … I can be really hard on myself, which also originates from my childhood … I am also the person who constantly takes responsibility and thinks ahead.”(Pregnant woman, interview 12)
“I prefer a high level of control … so when I lose control, I don’t always handle it well … as a child I was always in control of what happened at home because I, to a large extent, took care of things.”(Pregnant woman, interview 11)
“It’s quite anxiety-provoking that I am in the middle of something (being pregnant) that I am not able to control in any way. I don’t know what is ahead and that is really difficult.”(Pregnant woman, interview 8)
“… I need to prepare myself mentally for how to handle things. I have a really hard time when things change and I am unprepared…”(Pregnant woman, interview 5)
“It has been a great challenge for me to accept that there is something in my body I can’t control, something that grows, and that has its own life…”(Pregnant woman, interview 7)
“… my bodily change, the physical change…I have to weigh myself during pregnancy…my weight has been something I have previously been able to control…It triggers my need for control … I need to put on weight, this makes it really difficult…”(Pregnant woman, interview 8)
3.2.4. Anxiety Regarding Childbirth and Doubts of Motherhood Abilities
“… you meet other first time mothers and you are able to share and talk about your concerns…you also get different tools to help you breathe and relax … it has given me more confidence that I have acquired knowledge and experience…”(Pregnant woman, interview 9)
“… I used to look forward to the birth but now where it gets closer, I get somewhat nervous … I haven’t talked to anyone about it…”(Pregnant woman, interview 1)
“I mostly look forward to when it’s over (the birth), but I also fear it … When you go into labour, you can’t stop it, and you don’t know what it is like before you try it … it’s extremely hard for me.”(Pregnant woman, interview 8)
“I try not to think about it, because if I do … it gets out of control … so the less I think about it the better it will be … I haven’t talked to my midwife about this…”(Pregnant woman, interview 4)
“I have been concerned about whether I will be a good mother. Am I carrying too much emotional baggage which will affect the baby?… It makes me upset because it is really hard … As a person, my mood varies a lot … Will I become a parent like my parents?”(Pregnant woman, interview 3)
“I have been extremely mentally affected by the pregnancy … more than I had expected … even though this is a planned pregnancy … I am really worried about everything changing … that things are unpredictable … that I will see a shift in my identity … What if my boyfriend and I split up? What if we can’t handle it … Your whole existence changes, when you become a mother … I can accept that I am expecting a baby, but I have more difficulties imagining myself as a mother…”(Pregnant woman, interview 12)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Socialstyrelsen. Børn i Familier Med Misbrug. Available online: https://socialstyrelsen.dk/born/born-i-familier-i-familier-med-misbrug (accessed on 21 August 2021).
- Haugland, S.H.; Elgán, T.H. Prevalence of Parental Alcohol Problems among a General Population Sample of 28,047 Norwegian Adults: Evidence for a Socioeconomic Gradient. Int. J. Environ. Res. Public Health 2021, 18, 5412. [Google Scholar] [CrossRef]
- Pisinger, V.S.C.; Bloomfield, K.; Tolstrup, J.S. Perceived parental alcohol problems, internalizing problems and impaired parent—Child relationships among 71,988 young people in Denmark: Perceived parental alcohol problems. Addiction 2016, 111, 1966–1974. [Google Scholar] [CrossRef] [Green Version]
- Pisinger, V.S.C.; Hawton, K.; Tolstrup, J.S. Self-injury and suicide behavior among young people with perceived parental alcohol problems in Denmark: A school-based survey. Eur. Child Adolesc. Psychiatry 2018, 27, 201–208. [Google Scholar] [CrossRef]
- Balsa, A.I.; Homer, J.F.; French, M.T. The health effects of parental problem drinking on adult children. J. Ment. Health Policy Econ. 2009, 12, 55–66. [Google Scholar]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e356–e366. [Google Scholar] [CrossRef] [Green Version]
- Klostermann, K.; Chen, R.; Kelley, M.L.; Schroeder, V.M.; Braitman, A.L.; Mignone, T. Coping Behavior and Depressive Symptoms in Adult Children of Alcoholics. Subst. Use Misuse 2011, 46, 1162–1168. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Isobel, S.; Goodyear, M.; Furness, T.; Foster, K. Preventing intergenerational trauma transmission: A critical interpretive synthesis. J. Clin. Nurs. 2018, 28, 1100–1113. [Google Scholar] [CrossRef]
- Johnson, A.K.; Fulco, C.J.; Augustyn, M.B. Intergenerational continuity in alcohol misuse: Maternal alcohol use disorder and the sequelae of maternal and family functioning. Psychol. Addict. Behav. 2019, 33, 442–456. [Google Scholar] [CrossRef] [PubMed]
- Kerr, D.C.R.; Capaldi, D.M.; Pears, K.C.; Owen, L.D. Intergenerational influences on early alcohol use: Independence from the problem behavior pathway. Dev. Psychopathol. 2012, 24, 889–906. [Google Scholar] [CrossRef] [Green Version]
- Væver, M.S. Tidlig opsporing af psykisk mistrivsel hos spædbørn. Samfundsøkonomen 2018, 1, 29–31. [Google Scholar]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Muzik, M. Prenatal Attachment, Parental Confidence, and Mental Health in Expecting Parents: The Role of Childhood Trauma. J. Midwifery Women’s Health 2020, 65, 85–95. [Google Scholar] [CrossRef]
- Olsen, J.M. Integrative Review of Pregnancy Health Risks and Outcomes Associated With Adverse Childhood Experiences. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 783–794. [Google Scholar] [CrossRef]
- Young-Wolff, K.C.; Wei, J.; Varnado, N.; Rios, N.; Staunton, M.; Watson, C. Adverse Childhood Experiences and Pregnancy Intentions among Pregnant Women Seeking Prenatal Care. Womens Health Issues 2021, 31, 100–106. [Google Scholar] [CrossRef]
- Racine, N.; Madigan, S.; Plamondon, A.; Hetherington, E.; McDonald, S.; Tough, S. Maternal adverse childhood experiences and antepartum risks: The moderating role of social support. Arch. Women’s Ment. Health 2018, 21, 663–670. [Google Scholar] [CrossRef]
- Racine, N.; Zumwalt, K.; McDonald, S.; Tough, S.; Madigan, S. Perinatal depression: The role of maternal adverse childhood experiences and social support. J. Affect. Disord. 2020, 263, 576–581. [Google Scholar] [CrossRef]
- Wajid, A.; van Zanten, S.V.; Mughal, M.K.; Biringer, A.; Austin, M.P.; Vermeyden, L.; Kingston, D. Adversity in childhood and depression in pregnancy. Arch. Women’s Ment. Health 2020, 23, 169–180. [Google Scholar] [CrossRef]
- Savage, L.-É.; Tarabulsy, G.M.; Pearson, J.; Collin-Vézina, D.; Gagné, L.-M. Maternal history of childhood maltreatment and later parenting behavior: A meta-analysis. Dev. Psychopathol. 2019, 31, 9–21. [Google Scholar] [CrossRef]
- Brodén, M. Graviditetens Muligheder: En Tid Hvor Relationer Skabes Og Udvikles; Akademisk Forlag Kbh: Copenhagen, Denmark, 2018. [Google Scholar]
- Campbell, F.; Conti, G.; Heckman, J.J.; Moon, S.H.; Pinto, R.; Pungello, E.; Pan, Y. Early Childhood Investments Substantially Boost Adult Health. Science 2014, 343, 1478–1485. [Google Scholar] [CrossRef] [Green Version]
- København, S. (Ed.) National Board of Health. In Recommendations for Antenatal Care; The National Board of Health: Copenhagen, Denmark, 2021; pp. 1–212. [Google Scholar]
- The Ministry of Health. LBK nr 903 af 26/08/2019. The National Health Act. Available online: https://www.retsinformation.dk/Forms/R0710.aspx?id=210110 (accessed on 15 October 2021).
- Johnsen, H.; Christensen, U.; Juhl, M.; Villadsen, S.F. Organisational barriers to implementing the MAMAACT intervention to improve maternity care for non-Western immigrant women: A qualitative evaluation. Int. J. Nurs. Stud. 2020, 111, 103742. [Google Scholar] [CrossRef]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research, 3rd ed.; SAGE: Los Angeles, CA, USA, 2014. [Google Scholar]
- Kvale, S.; Brinkmann, S. Interview: Det Kvalitative Forskningsinterview Som Håndværk; Hans Reitzels Forlag: København, Denmark, 2014. [Google Scholar]
- Malterud, K. Kvalitative Forskningsmetoder for Medisin Og Helsefag: En Innføring; Universitetsforlaget: Oslo, Norway, 2017. [Google Scholar]
- National Committee on Health Research Ethics. What to Notify. Available online: https://en.nvk.dk/how-to-notify/what-to-notify (accessed on 21 August 2021).
- Haverfield, M.C.; Theiss, J.A. A theme analysis of experiences reported by adult children of alcoholics in online support forums. J. Fam. Stud. 2014, 20, 166–184. [Google Scholar] [CrossRef]
- Lindquist, A.; Kurinczuk, J.J.; Redshaw, M.; Knight, M. Experiences, utilisation and outcomes of maternity care in England among women from different socio-economic groups: Findings from the 2010 National Maternity Survey. BJOG 2015, 122, 1610–1617. [Google Scholar] [CrossRef] [PubMed]
- Morozumi, R.; Matsumura, K.; Hamazaki, K.; Tsuchida, A.; Takamori, A.; Inadera, H. Impact of individual and neighborhood social capital on the physical and mental health of pregnant women: The Japan Environment and Children’s Study (JECS). BMC Pregnancy Childbirth 2020, 20, 450. [Google Scholar] [CrossRef]
- Due, P. Social relations: Network, support and relational strain. Soc. Sci. Med. 1999, 48, 661–673. [Google Scholar] [CrossRef]
- Järvinen, M. Understanding Addiction: Adult Children of Alcoholics Describing Their Parents’ Drinking Problems. J. Fam. Issues 2015, 36, 805–825. [Google Scholar] [CrossRef] [Green Version]
- Shim, J.K. Cultural Health Capital: A Theoretical Approach to Understanding Health Care Interactions and the Dynamics of Unequal Treatment. J. Health Soc. Behav. 2010, 51, 1–15. [Google Scholar] [CrossRef]
- Peñacoba-Puente, C.; Monge, F.J.C.; Morales, D.M. Pregnancy worries: A longitudinal study of Spanish women: Evolution of worries over pregnancy. Acta Obstet. Gynecol. Scand. 2011, 90, 1030–1035. [Google Scholar] [CrossRef]
- Eide, J.; Hovengen, R.; Nordhagen, R. Childhood abuse and later worries about the baby’s health in pregnancy. Acta Obstet. Gynecol. Scand. 2010, 89, 1523–1531. [Google Scholar] [CrossRef]
- World Health Organization. Adverse Childhood Experiences International Questionnaire. In Pilot Study Review and Finalization Meeting, 4–5 May; WHO Headquarters: Geneva, Switzerland, 2011. [Google Scholar]
- Ångerud, K.; Annerbäck, E.-M.; Tydén, T.; Boddeti, S.; Kristiansson, P. Adverse childhood experiences and depressive symptomatology among pregnant women. Acta Obstet. Gynecol. Scand. 2018, 97, 701–708. [Google Scholar] [CrossRef] [Green Version]
- Moghaddam Hosseini, V.; Nazarzadeh, M.; Jahanfar, S. Interventions for reducing fear of childbirth: A systematic review and meta-analysis of clinical trials. Women Birth 2018, 31, 254–262. [Google Scholar] [CrossRef]
- Cassidy, J.; Brett, B.E.; Gross, J.T.; Stern, J.A.; Martin, D.R.; Mohr, J.J.; Woodhouse, S.S. Circle of Security–Parenting: A randomized controlled trial in Head Start. Dev. Psychopathol. 2017, 29, 651–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; The World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Rayment-Jones, H.; Murrells, T.; Sandall, J. An investigation of the relationship between the caseload model of midwifery for socially disadvantaged women and childbirth outcomes using routine data—A retrospective, observational study. Midwifery 2015, 31, 409–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beake, S.; Acosta, L.; Cooke, P.; McCourt, C. Caseload midwifery in a multi-ethnic community: The women’s experiences. Midwifery 2013, 29, 996–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jepsen, I.; Mark, E.; Nøhr, E.A.; Foureur, M.; Sørensen, E.E. A qualitative study of how caseload midwifery is constituted and experienced by Danish midwives. Midwifery 2016, 36, 61–69. [Google Scholar] [CrossRef]
- Jepsen, I.; Juul, S.; Foureur, M.; Sørensen, E.E.; Nøhr, E.A. Is caseload midwifery a healthy work-form?—A survey of burnout among midwives in Denmark. Sex. Reprod. Healthc. 2017, 11, 102–106. [Google Scholar] [CrossRef]
- Patton, M.Q. Enhancing the quality and credibility of qualitative analysis. Health Serv. Res. 1999, 34 (5 Pt 2), 1189–1208. [Google Scholar]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnsen, H.; Juhl, M.; Møller, B.K.; de Lichtenberg, V. Adult Daughters of Alcoholic Parents—A Qualitative Study of These Women’s Pregnancy Experiences and the Potential Implications for Antenatal Care Provision. Int. J. Environ. Res. Public Health 2022, 19, 3714. https://doi.org/10.3390/ijerph19063714
Johnsen H, Juhl M, Møller BK, de Lichtenberg V. Adult Daughters of Alcoholic Parents—A Qualitative Study of These Women’s Pregnancy Experiences and the Potential Implications for Antenatal Care Provision. International Journal of Environmental Research and Public Health. 2022; 19(6):3714. https://doi.org/10.3390/ijerph19063714
Chicago/Turabian StyleJohnsen, Helle, Mette Juhl, Bodil Kirstine Møller, and Vibeke de Lichtenberg. 2022. "Adult Daughters of Alcoholic Parents—A Qualitative Study of These Women’s Pregnancy Experiences and the Potential Implications for Antenatal Care Provision" International Journal of Environmental Research and Public Health 19, no. 6: 3714. https://doi.org/10.3390/ijerph19063714